Brain Activation Evoked by Sensory Stimulation in Patients with Spinal Cord Injury : Functional Magnetic Resonance Imaging Correlations with Clinical Features
- Affiliations
-
- 1Department of Neurosurgery, College of Medicine, Inha University, Incheon, Korea. nsyoon@gmail.com
- 2Department of Neurosurgery, Guro Cham Teun Teun Hospital, Seoul, Korea.
- KMID: 2191374
- DOI: http://doi.org/10.3340/jkns.2015.58.3.242
Abstract
OBJECTIVE
The purpose of this study is to determine whether the changes of contralateral sensorimotor cortical activation on functional magnetic resonance imaging (fMRI) can predict the neurological outcome among spinal cord injury (SCI) patients when the great toes are stimulated without notice.
METHODS
This study enrolled a total of 49 patients with SCI and investigated each patient's preoperative fMRI, postoperative fMRI, American Spinal Injury Association (ASIA) score, and neuropathic pain occurrence. Patients were classified into 3 groups according to the change of blood oxygenation level dependent (BOLD) response on perioperative fMRI during proprioceptive stimulation with repetitive passive toe movements : 1) patients with a response of contralateral sensorimotor cortical activation in fMRI were categorized; 2) patients with a response in other regions; and 3) patients with no response. Correlation between the result of fMRI and each parameter was analyzed.
RESULTS
In fMRI data, ASIA score was likely to show greater improvement in patients in group A compared to those belonging to group B or C (p<0.001). No statistical significance was observed between the result of fMRI and neuropathic pain (p=0.709). However, increase in neuropathic pain in response to the signal change of the ipsilateral frontal lobe on fMRI was statistically significant (p=0.030).
CONCLUSION
When there was change of BOLD response at the contralateral sensorimotor cortex on perioperative fMRI after surgery, relief of neurological symptoms was highly likely for traumatic SCI patients. In addition, development of neuropathic pain was likely to occur when there was change of BOLD response at ipsilateral frontal lobe.
MeSH Terms
Figure
-
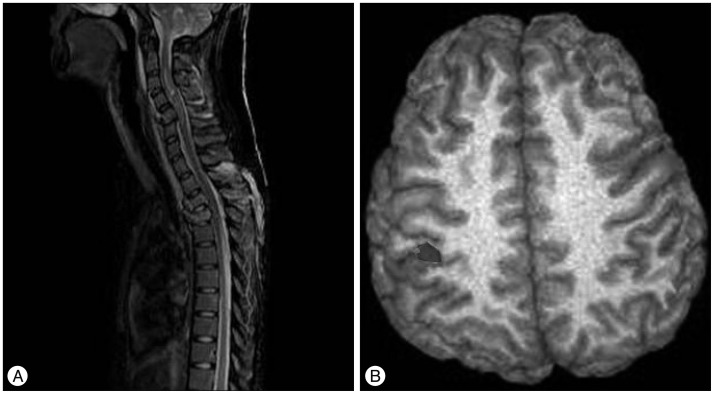
Fig. 1 An 18-year-old female was admitted after an automobile accident, and was confirmed to have initial ASIA score A (C4 level). A : On the initial spinal MRI, bursting fractures of C5, T3, and T4, as well as severe cord contusion were found. B : Functional MRI (fMRI) was taken 3 months after anterior and posterior fixation surgery. On the fMRI, a signal change was observed in the contralateral primary sensorimotor cortex. After surgery and 6 months conservative treatment, the ASIA score was upgraded to ASIA score B. Her follow up period was 20 months and there was no further improvement. ASIA : American Spinal Injury Association.
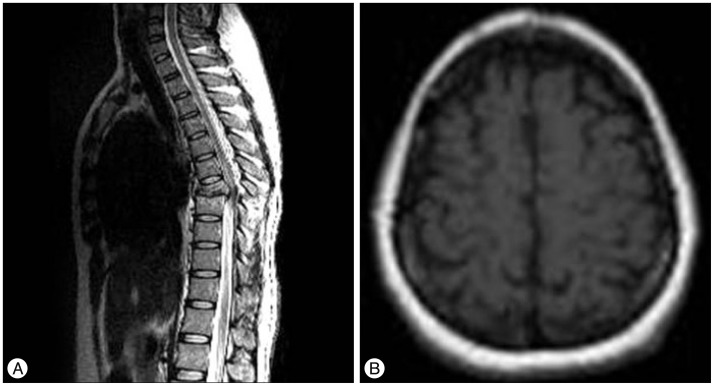
Fig. 2 A 40-year-old female was admitted to this hospital after a pedestrian traffic accident. She was confirmed to have initial ASIA score B (T8 level). A : On the initial spinal MRI, T7 bursting fracture, dislocation, and severe cord contusion were found. B : Functional MRI (fMRI) was taken 2 weeks after posterior decompression and fixation surgery. There was no positive signal in the postoperative fMRI data, despite surgery and treatment. Despite follow up of 20 months, there was no neurologic improvement. ASIA : American Spinal Injury Association.

Fig. 3 A 41-year-old male was admitted after falling from a height of 5 meters. He was confirmed to have ASIA score A (T12 level). A : On the initial spinal MRI, T12 bursting fracture, dislocation, and severe cord contusion were found. B : Functional MRI (fMRI) was taken 1 week after posterior decompression and fixation surgery. In the fMRI data, there was a signal change in the ipsilateral frontal lobe. After surgery, he was followed up for 36 months, but there was no improvement of follow-up ASIA score. EMG and EP showed no abnormality, but he continued to have neuropathic pain. ASIA : American Spinal Injury Association, EMG : electromyography, EP : electrophysiology study.
Reference
-
1. Bazley FA, Hu C, Maybhate A, Pourmorteza A, Pashai N, Thakor NV, et al. Electrophysiological evaluation of sensory and motor pathways after incomplete unilateral spinal cord contusion. J Neurosurg Spine. 2012; 16:414–423. PMID: 22303873.
Article2. Curt A, Bruehlmeier M, Leenders KL, Roelcke U, Dietz V. Differential effect of spinal cord injury and functional impairment on human brain activation. J Neurotrauma. 2002; 19:43–51. PMID: 11852977.
Article3. Curt A, Dietz V. Electrophysiological recordings in patients with spinal cord injury : significance for predicting outcome. Spinal Cord. 1999; 37:157–165. PMID: 10213324.
Article4. Duggal N, Rabin D, Bartha R, Barry RL, Gati JS, Kowalczyk I, et al. Brain reorganization in patients with spinal cord compression evaluated using fMRI. Neurology. 2010; 74:1048–1054. PMID: 20200344.
Article5. Freund P, Weiskopf N, Ashburner J, Wolf K, Sutter R, Altmann DR, et al. MRI investigation of the sensorimotor cortex and the corticospinal tract after acute spinal cord injury : a prospective longitudinal study. Lancet Neurol. 2013; 12:873–881. PMID: 23827394.
Article6. Haanpää M, Attal N, Backonja M, Baron R, Bennett M, Bouhassira D, et al. NeuPSIG guidelines on neuropathic pain assessment. Pain. 2011; 152:14–27. PMID: 20851519.
Article7. Henwood P, Ellis JA. Chronic neuropathic pain in spinal cord injury : the patient's perspective. Pain Res Manag. 2004; 9:39–45. PMID: 15007402.
Article8. Jacobs SR, Yeaney NK, Herbison GJ, Ditunno JF Jr. Future ambulation prognosis as predicted by somatosensory evoked potentials in motor complete and incomplete quadriplegia. Arch Phys Med Rehabil. 1995; 76:635–641. PMID: 7605182.
Article9. Jung JK, Oh CH, Yoon SH, Ha Y, Park S, Choi B. Outcome evaluation with signal activation of functional MRI in spinal cord injury. J Korean Neurosurg Soc. 2011; 50:209–215. PMID: 22102951.
Article10. Lotze M, Laubis-Herrmann U, Topka H, Erb M, Grodd W. Reorganization in the primary motor cortex after spinal cord injury - a functional Magnetic Resonance (fMRI) study. Restor Neurol Neurosci. 1999; 14:183–187.11. Masri R, Keller A. Chronic pain following spinal cord injury. Adv Exp Med Biol. 2012; 760:74–88. PMID: 23281514.
Article12. McDonald JW, Becker D, Holekamp TF, Howard M, Liu S, Lu A, et al. Repair of the injured spinal cord and the potential of embryonic stem cell transplantation. J Neurotrauma. 2004; 21:383–393. PMID: 15115588.
Article13. Rocca MA, Agosta F, Martinelli V, Falini A, Comi G, Filippi M. The level of spinal cord involvement influences the pattern of movement-associated cortical recruitment in patients with isolated myelitis. Neuroimage. 2006; 30:879–884. PMID: 16307896.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Traumatic Atypical Tetraplegia Without Radiologic Abnormalities Including Magnetic Resonance Imaging in an Adult: A Case Report
- Effects of Functional Magnetic Stimulation on the Functional Recovery in a Rat Model of Spinal Cord Injury
- Comparative Study of Functional Magnetic Resonance Imaging by Global Scaling Analysis
- Features of the Myelopathy in Patients with Electrical Burn
- Motor Evoked Potentials in Transverse Myelitis
