Eleven Year's Single Center Experience of Endovascular Treatment of Anterior Communicating Artery Aneurysms: Focused on Digital Subtraction Angiography Follow-Up Results
- Affiliations
-
- 1Department of Neurosurgery, Medical Research Institute, Pusan National University School of Medicine, University Pusan National University Hospital, Busan, Korea. medifirst@pusan.ac.kr
- 2Department of Diagnostic Radiology, Medical Research Institute, Pusan National University School of Medicine, University Pusan National University Hospital, Busan, Korea.
- 3Department of Diagnostic Radiology, Busan Paik Hospital, Inje University College of Medicine, Busan, Korea.
- KMID: 2191356
- DOI: http://doi.org/10.3340/jkns.2015.58.3.184
Abstract
OBJECTIVE
Anterior communicating artery (AcomA) aneurysms represent the most common intracranial aneurysms and challenging to treat due to complex vascularity. The purpose of this study was to report our experience of endovascular treatment of AcomA aneurysms.
METHODS
Between January 2003 and December 2013, we retrospectively reviewed the medical records of 134 AcomA aneurysm patients available more than 6 months conventional angiographic and clinical follow-up results. We focused on aneurismal or AcomA vascular characters, angiographic and clinical follow-up results, and retreatment.
RESULTS
The rate of ruptured cases was 75.4%, and the small (<10 mm) aneurysms were 96.3%. Based on the subtypes defined by dominance of A1, 79 patients (59%) had contralateral A1 hypoplasia or agenesis. The immediate post-procedural angiography confirmed complete occlusion in 75.4%, partial occlusion in 24.6%. Procedure related complications were observed in 25 (18.6%) patients. Most of the adverse events were asymptomatic. Follow-up conventional angiography at > or =6 months was performed in all patients (mean 16.3 months) and major recanalization was noted in 6.7% and regrowth in one case. The aneurysm size (p=0.016), and initial treatment results (p=0.00) were statistically significant risk factors related to aneurysm recurrence. An overall improvement in mRS was observed during the clinical follow-up period and no rebleeding episode occurred.
CONCLUSION
This study demonstrated that endovascular treatment is an effective treatment modality for AcomA aneurysms with low morbidity. Patients should take long term clinical and angiographic follow-up in order to assess the recurrence and warrant retreatment, especially ruptured, large, and initially incomplete occluded aneurysms.
MeSH Terms
Figure
-
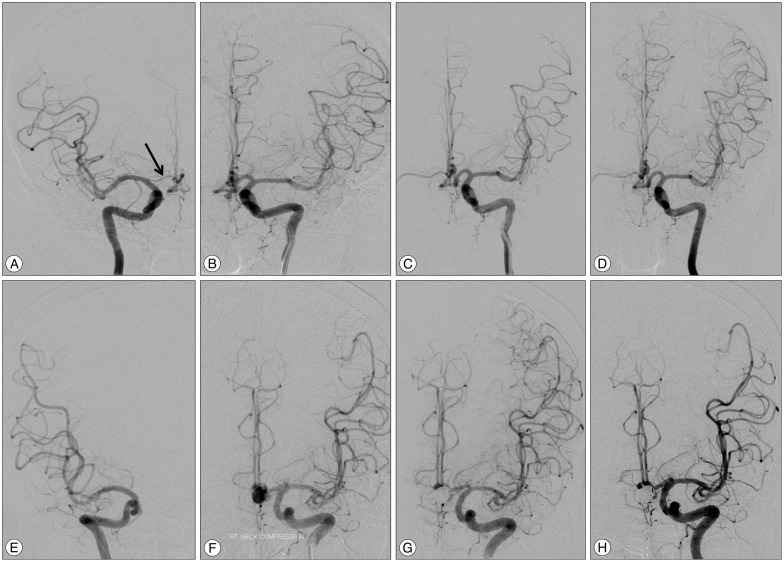
Fig. 1 Images of anterior communicating artery aneurysms with contralateral A1 hypoplasia (A-D) and agenesis (E-H). A and B : Right and left internal carotid artery angiographies demonstrate left anterior communicating artery aneurysm with right A1 hypoplasia (black arrow). C : Final image after coiling shows complete occlusion of the aneurysm. D : The 6 months follow-up angiogram confirms stable occlusion of the coiled aneurysm. E and F : Both internal carotid arteries digital subtraction angiographies shows left anterior communicating artery aneurysm with contralateral A1 agenesis. G and H : Angiography immediately after coiling and 2 years follow-up image confirms complete and stable occlusion of the aneurysm sac.
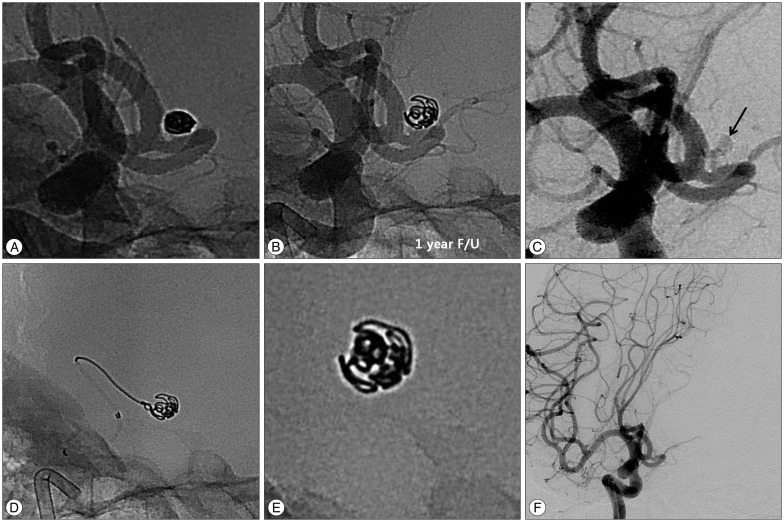
Fig. 2 Retreatment of a 51-years-old female patient with recurred aneurysm. A : Initial unsubtracted image of conventional angiography shows complete occlusion of an aneurysm sac. B : Unsubtracted image of 1 year follow-up demonstrates enlarged and loosened coil mass. C : Subtracted image of previously coiled aneurysm reveals contrast filling of the aneurysm sac (black arrow, regrowth). D : Retreatment of recurred aneurysm using simple coiling technique. E : X-ray image of retreated coil mass. F : Final angiography after retreatment demonstrates complete occlusion of the recurred aneurysm.
Reference
-
1. Byrne JV, Sohn MJ, Molyneux AJ, Chir B. Five-year experience in using coil embolization for ruptured intracranial aneurysms : outcomes and incidence of late rebleeding. J Neurosurg. 1999; 90:656–663. PMID: 10193610.
Article2. Campi A, Ramzi N, Molyneux AJ, Summers PE, Kerr RS, Sneade M, et al. Retreatment of ruptured cerebral aneurysms in patients randomized by coiling or clipping in the International Subarachnoid Aneurysm Trial (ISAT). Stroke. 2007; 38:1538–1544. PMID: 17395870.
Article3. Cognard C, Weill A, Spelle L, Piotin M, Castaings L, Rey A, et al. Long-term angiographic follow-up of 169 intracranial berry aneurysms occluded with detachable coils. Radiology. 1999; 212:348–356. PMID: 10429689.
Article4. Corns R, Zebian B, Tait MJ, Walsh D, Hampton T, Deasy N, et al. Prevalence of recurrence and retreatment of ruptured intracranial aneurysms treated with endovascular coil occlusion. Br J Neurosurg. 2013; 27:30–33. PMID: 22762269.
Article5. Fang S, Brinjikji W, Murad MH, Kallmes DF, Cloft HJ, Lanzino G. Endovascular treatment of anterior communicating artery aneurysms : a systematic review and meta-analysis. AJNR Am J Neuroradiol. 2014; 35:943–947. PMID: 24287090.
Article6. Finitsis S, Anxionnat R, Lebedinsky A, Albuquerque PC, Clayton MF, Picard L, et al. Endovascular treatment of ACom intracranial aneurysms. Report on series of 280 patients. Interv Neuroradiol. 2010; 16:7–16. PMID: 20377974.
Article7. Gallas S, Januel AC, Pasco A, Drouineau J, Gabrillargues J, Gaston A, et al. Long-term follow-up of 1036 cerebral aneurysms treated by bare coils : a multicentric cohort treated between 1998 and 2003. AJNR Am J Neuroradiol. 2009; 30:1986–1992. PMID: 19679641.
Article8. Gonzalez N, Sedrak M, Martin N, Vinuela F. Impact of anatomic features in the endovascular embolization of 181 anterior communicating artery aneurysms. Stroke. 2008; 39:2776–2782. PMID: 18617670.
Article9. Henkes H, Fischer S, Liebig T, Weber W, Reinartz J, Miloslavski E, et al. Repeated endovascular coil occlusion in 350 of 2759 intracranial aneurysms safety and effectiveness aspects. Neurosurgery. 2006; 58:224–232. discussion 224-232PMID: 16462475.
Article10. Higashida R, Furlan A, Roberts H, Tomsick T, Connors B, Barr J, et al. Trial design and reporting standards for intraarterial cerebral thrombolysis for acute ischemic stroke. J Vasc Interv Radiol. 2003; 14(9 Pt 2):S493–S494. PMID: 14514864.
Article11. Kwon SC, Kwon OK. Korean Unruptured Cerebral Aneurysm Coiling (KUCAC) Investigators. Endovascular coil embolization of unruptured intracranial aneurysms : a Korean multicenter study. Acta Neurochir (Wien). 2014; 156:847–854. PMID: 24610449.
Article12. Li H, Pan R, Wang H, Rong X, Yin Z, Milgrom DP, et al. Clipping versus coiling for ruptured intracranial aneurysms : a systematic review and meta-analysis. Stroke. 2013; 44:29–37. PMID: 23238862.
Article13. Molyneux A, Kerr R, Stratton I, Sandercock P, Clarke M, Shrimpton J, et al. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms : a randomised trial. Lancet. 2002; 360:1267–1274. PMID: 12414200.
Article14. Moret J, Pierot L, Boulin A, Castaings L, Rey A. Endovascular treatment of anterior communicating artery aneurysms using Guglielmi detachable coils. Neuroradiology. 1996; 38:800–805. PMID: 8957810.
Article15. Nathal E, Yasui N, Sampei T, Suzuki A. Intraoperative anatomical studies in patients with aneurysms of the anterior communicating artery complex. J Neurosurg. 1992; 76:629–634. PMID: 1545257.
Article16. Ogungbo B, Gregson BA, Blackburn A, Mendelow AD. Newcastle Subarachnoid Study Group. Trends over time in the management of subarachnoid haemorrhage in newcastle : review of 1609 patients. Br J Neurosurg. 2001; 15:388–395. PMID: 11708541.
Article17. Perlmutter D, Rhoton AL Jr. Microsurgical anatomy of the anterior cerebral-anterior communicating-recurrent artery complex. J Neurosurg. 1976; 45:259–272. PMID: 948013.
Article18. Raymond J, Guilbert F, Weill A, Georganos SA, Juravsky L, Lambert A, et al. Long-term angiographic recurrences after selective endovascular treatment of aneurysms with detachable coils. Stroke. 2003; 34:1398–1403. PMID: 12775880.
Article19. Raymond J, Kotowski M, Darsaut TE, Molyneux AJ, Kerr RS. Ruptured aneurysms and the International Subarachnoid Aneurysm Trial(ISAT): What is known and what remains to be questioned. Neurochirurgie. 2012; 58:103–114. PMID: 22481029.
Article20. Renowden SA, Koumellis P, Benes V, Mukonoweshuro W, Molyneux AJ, McConachie NS. Retreatment of previously embolized cerebral aneurysms : the risk of further coil embolization does not negate the advantage of the initial embolization. AJNR Am J Neuroradiol. 2008; 29:1401–1404. PMID: 18436614.
Article21. Ries T, Siemonsen S, Thomalla G, Grzyska U, Zeumer H, Fiehler J. Long-term follow-up of cerebral aneurysms after endovascular therapy prediction and outcome of retreatment. AJNR Am J Neuroradiol. 2007; 28:1755–1761. PMID: 17885238.
Article22. Roy D, Milot G, Raymond J. Endovascular treatment of unruptured aneurysms. Stroke. 2001; 32:1998–2004. PMID: 11546888.
Article23. Sim JH. Intracranial aneurysms in Korea. Neurol Med Chir (Tokyo). 1998; 38(Suppl):118–121. PMID: 10234990.
Article24. Stehbens WE. Aneurysms and anatomical variation of cerebral arteries. Arch Pathol. 1963; 75:45–64. PMID: 14087271.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Rupture Risk of Aneurysm in the Anterior Communicating Artery: A Single Center Study
- Multiple Separate Aneurysms on Anterior Communicating Artery
- Rupture of De Novo Anterior Communicating Artery Aneurysm 8 Days after the Clipping of Ruptured Middle Cerebral Artery Aneurysm
- Three-Dimensional Digital Subtraction Angiographic Evaluation of Aneurysm Remnants after Clip Placement
- Variations and anomalies of the circle of Willis in Korean: Cerebral digital subtraction angiogram studies in 200 cases
