Quantitative Evaluation of Median Nerve Motor Function in Carpal Tunnel Syndrome Using Load Cell : Correlation with Clinical, Electrodiagnostic, and Ultrasonographic Findings
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University College of Medicine, Seoul, Korea.
- 2Department of Neurosurgery, Seoul National University Boramae Hospital, Seoul, Korea. nsyang@brm.co.kr
- 3Interdisciplinary Program of Bioengineering, Seoul National University, Seoul, Korea.
- KMID: 2190903
- DOI: http://doi.org/10.3340/jkns.2013.54.3.232
Abstract
OBJECTIVE
Major complaints of carpal tunnel syndrome (CTS) are sensory components. However, motor deficit also impedes functional status of hand. Contrary to evaluation of sensory function, the objective, quantitative evaluation of median nerve motor function is not easy. The motor function of median was evaluated quantitatively using load cell and its correlation with findings of electrodiagnostic study (EDS) was evaluated.
METHODS
Objective motor function of median nerve was evaluated by load cell and personal computer-based measurement system. All of the measurement was done in patients diagnosed as having idiopathic CTS by clinical features and EDS findings. The strength of thumb abduction and index finger flexion was measured in each hand three times, and the average value was used to calculate thumb index ratio (TIR). The correlation of TIR with clinical, EDS, and ultrasonographic findings were evaluated.
RESULTS
The TIR was evaluated in 67 patients (119 hands). There were 14 males and 53 females, mean age were 57.6 years (range 28 to 81). The higher preoperative nerve conductive studies grade of the patients, the lower TIR was observed [p<0.001, analysis of variance (ANOVA)]. TIR of cases with thenar atrophy were significantly lower than those without (p<0.001, t-test). TIR were significantly lower in patients with severe median nerve swelling in ultrasonography (p=0.042, ANOVA).
CONCLUSION
Measurements of median nerve motor function using load cell is a valuable evaluation tool in CTS. It might be helpful in detecting subclinical motor dysfunction before muscle atrophy develops.
Keyword
MeSH Terms
Figure
-
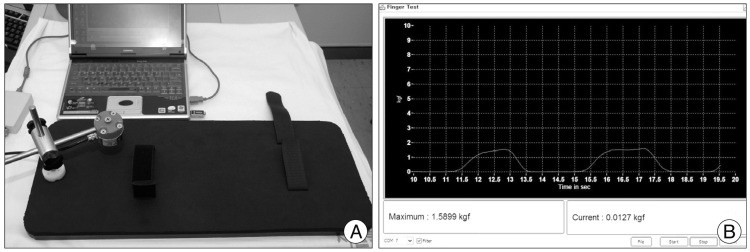
Fig. 1 Device and program for measuring thumb abduction strength. The device (A) is composed of base plate with velcro strap, load cell mounted on adjustable arm. The screen capture (B) shows graphic output of measured muscle strength in kilogram force.
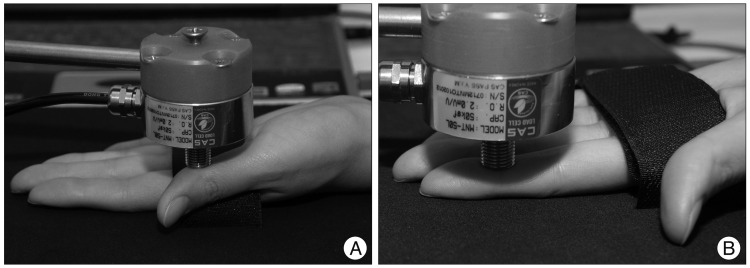
Fig. 2 The measurement of thumb abduction and index flexion strength. Thumb abduction strength is measured by placing load cell at the radial border of the thumb interphalangeal joint flexion crease (A). Index flexion strength is measured by placing load cell at the distal interphalangeal joint flexion crease (B).
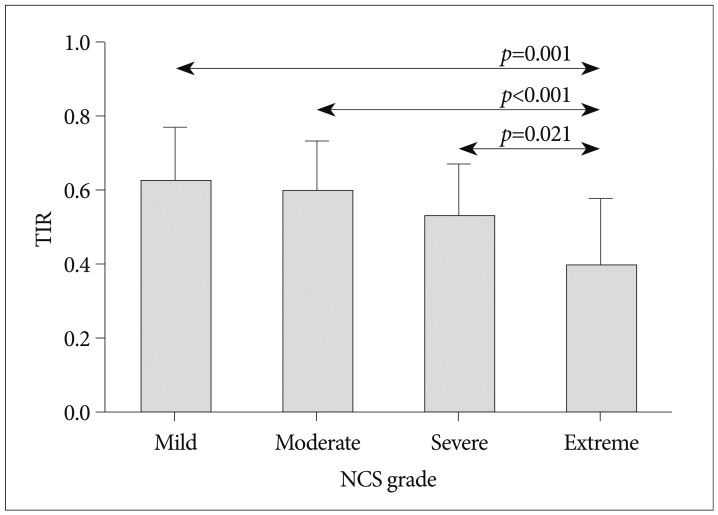
Fig. 3 The difference of TIR according to NCS grade. The TIR of NCS grade extremely severe was significantly lower than those of other NCS grades in post-hoc analysis. TIR : thumb index ratio, NCS : nerve conductive studies.
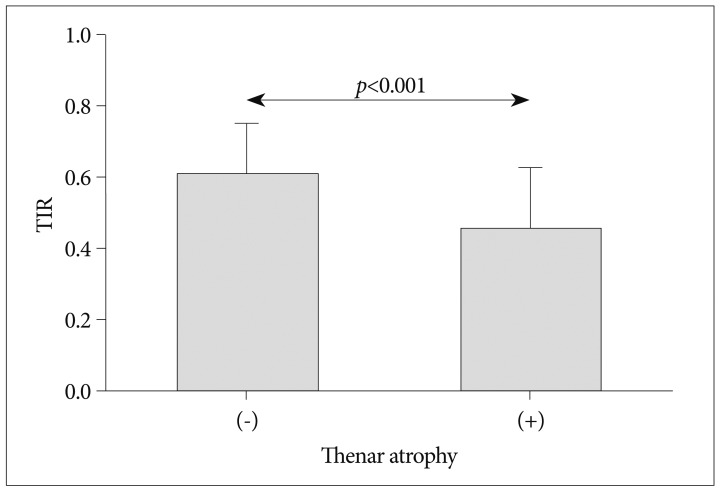
Fig. 4 The difference of TIR according to presence or absence of thenar atrophy on physical examination. TIR : thumb index ratio.
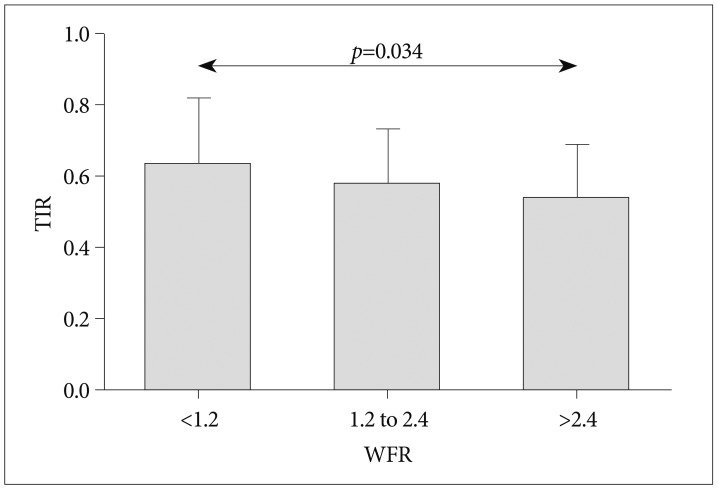
Fig. 5 The difference of TIR according to WFR. The patients with higher WFR have significantly lower TIR in post-hoc analysis (p=0.034). TIR : thumb index ratio, WFR : wrist to forearm ratio.
Reference
-
1. Agabegi SS, Freiberg RA, Plunkett JM, Stern PJ. Thumb abduction strength measurement in carpal tunnel syndrome. J Hand Surg Am. 2007; 32:859–866. PMID: 17606067.
Article2. Ahn SY, Hong YH, Koh YH, Chung YS, Lee SH, Yang HJ. Pressure measurement in carpal tunnel syndrome : correlation with electrodiagnostic and ultrasonographic findings. J Korean Neurosurg Soc. 2009; 46:199–204. PMID: 19844618.
Article3. Aroori S, Spence RA. Carpal tunnel syndrome. Ulster Med J. 2008; 77:6–17. PMID: 18269111.4. Crosby CA, Wehbé MA, Mawr B. Hand strength : normative values. J Hand Surg Am. 1994; 19:665–670. PMID: 7963331.5. Geere J, Chester R, Kale S, Jerosch-Herold C. Power grip, pinch grip, manual muscle testing or thenar atrophy - which should be assessed as a motor outcome after carpal tunnel decompression? A systematic review. BMC Musculoskelet Disord. 2007; 8:114. PMID: 18028538.
Article6. Jerosch-Herold C, Shepstone L, Miller L, Chapman P. The responsiveness of sensibility and strength tests in patients undergoing carpal tunnel decompression. BMC Musculoskelet Disord. 2011; 12:244. PMID: 22032626.
Article7. Liu F, Watson HK, Carlson L, Lown I, Wollstein R. Use of quantitative abductor pollicis brevis strength testing in patients with carpal tunnel syndrome. Plast Reconstr Surg. 2007; 119:1277–1283. PMID: 17496602.
Article8. Padua L, LoMonaco M, Gregori B, Valente EM, Padua R, Tonali P. Neurophysiological classification and sensitivity in 500 carpal tunnel syndrome hands. Acta Neurol Scand. 1997; 96:211–217. PMID: 9325471.
Article9. Schreuders TA, Roebroeck ME, Jaquet JB, Hovius SE, Stam HJ. Measuring the strength of the intrinsic muscles of the hand in patients with ulnar and median nerve injuries : reliability of the Rotterdam Intrinsic Hand Myometer (RIHM). J Hand Surg Am. 2004; 29:318–324. PMID: 15043908.
Article10. Shim CS, Kim GK, Lim YJ, Kim TS, Rhee BA, Leem W. A clinical analysis of the carpal tunnel syndrome. J Korean Neurosurg Soc. 1993; 22:364–370.11. Sunderland S. Nerve injuries and their repair. A critical appraisal. Edinburgh: Churcill Livingstone;1991.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Correlation Between Electrodiagnostic Results and Ultrasonographic Findings in the Severity of Carpal Tunnel Syndrome in Females
- Analysis of Sonographic Measurement by Anatomical Area in Carpal Tunnel Syndrome and Correlation the Measurement with Electrodiagnostic Study
- Ultrasonographic Study of Median Nerve after Carpal Tunnel Release
- Retrograde Changes of Median-Nerve Fibers in Carpal Tunnel Syndrome
- The Relationship between Clinical and Electrodiagnostic Findings in Carpal Tunnel Syndrome
