J Korean Neurosurg Soc.
2013 Jun;53(6):377-379. 10.3340/jkns.2013.53.6.377.
Large Perforation of Hypopharynx Secondary to Anterior Cervical Approach : A Complicated Case
- Affiliations
-
- 1Department of Otolaryngology Head and Neck Surgery, College of Medicine, Chosun University, Gwangju, Korea.
- 2Department of Neurosurgery, College of Medicine, Chosun University, Gwangju, Korea. chosunns@chosun.ac.kr
- 3Department of Neurosurgery, Heori Sarang Hospital, Daejeon, Korea.
- KMID: 2190829
- DOI: http://doi.org/10.3340/jkns.2013.53.6.377
Abstract
- Perforation of the hypopharynx, which can occur after anterior cervical approach, is a very rare type of complication. If diagnosed late, it can lead to very fatal course, such as mediastinitis and hematosepsis. Therefore, a precise and prompt diagnosis is crucial. When conservative treatment alone is not expected to heal the perforated site or is likely to lead to serious complications, surgical treatment becomes necessary. This report demonstrates that surgical intervention performed immediately after an early diagnosis can lead to the successful treatment of a large perforation in the hypopharynx on a 58-year-old male patient.
Keyword
Figure
-
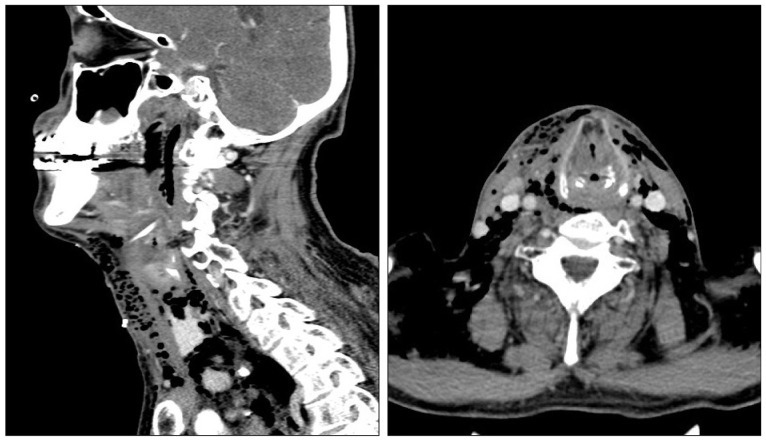
Fig. 1 Preoperative computed tomography scans show a large amount of subcutaneous emphysema in the anterior lateral cervical regions.
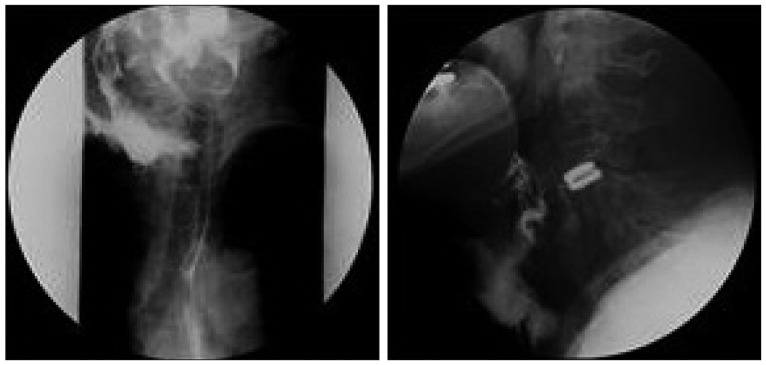
Fig. 2 Contrast study reveal a large fistulous tract and contrast leaking from the right pyriform sinus into the operation site.
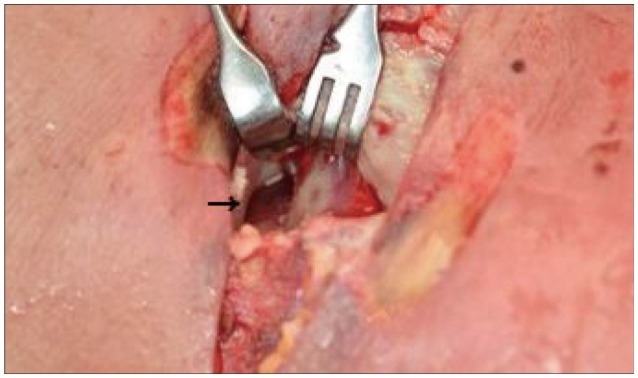
Fig. 3 A perforation approximately 2 cm long in the right hypopharynx (arrow). Severe inflammation can be observed in the surrounding region.

Fig. 4 Contrast study performed at 13th day after surgery reveal the leakage, which was observed before surgery is absent.
Reference
-
1. Buecker A, Wein BB, Neuerburg JM, Guenther RW. Esophageal perforation : comparison of use of aqueous and barium-containing contrast media. Radiology. 1997; 202:683–686. PMID: 9051016.
Article2. Endicott JN, Molony TB, Campbell G, Bartels LJ. Esophageal perforations : the role of computerized tomography in diagnosis and management decisions. Laryngoscope. 1986; 96:751–757. PMID: 3724326.3. Fountas KN, Kapsalaki EZ, Nikolakakos LG, Smisson HF, Johnston KW, Grigorian AA, et al. Anterior cervical discectomy and fusion associated complications. Spine (Phila Pa 1976). 2007; 32:2310–2317. PMID: 17906571.
Article4. Heater DW, Haskvitz L. Suspected pharyngoesophageal perforation after a difficult intubation : a case report. AANA J. 2005; 73:185–187. PMID: 16010770.5. Hinojar AG, Díaz Díaz MA, Pun YW, Hinojar AA. Management of hypopharyngeal and cervical oesophageal perforations. Auris Nasus Larynx. 2003; 30:175–182. PMID: 12753990.
Article6. Kras JF, Marchmont-Robinson H. Pharyngeal perforation during intubation in a patient with Crohn's disease. J Oral Maxillofac Surg. 1989; 47:405–407. PMID: 2926551.
Article7. Lee JS, Kang DH, Hwang SH, Han JW. Oral extrusion of screw after anterior cervical interbody fusion. J Korean Neurosurg Soc. 2008; 44:259–261. PMID: 19096688.
Article8. Lee TS, Jordan JS. Pyriform sinus perforation secondary to traumatic intubation in a difficult airway patient. J Clin Anesth. 1994; 6:152–155. PMID: 8204237.
Article9. Niezgoda JA, McMenamin P, Graeber GM. Pharyngoesophageal perforation after blunt neck trauma. Ann Thorac Surg. 1990; 50:615–617. PMID: 2222052.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Giant Fibrovascular Polyp of the Hypopharynx Removed by Transoral Approach
- Delayed Esophageal Perforation after Cervical Spine Plating
- Clinical Analysis of Anterior Approach with the Several Types of Cervical Plate for the Lower Cervical Lesions
- Acute Descending Necrotizing Mediastinitis Secondary to Spontaneous Rupture of Hypopharynx: A Case Report
- Early Detection of Anterior Cervical Osteophytes Causing Dysphagia by Esophagogastroduodenoscopy
