Mesenchymal chondrosarcoma on right mandible: a case report
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, School of Dentistry, Kyung Hee University, Seoul, Korea. leebs@khu.ac.kr
- KMID: 2189992
- DOI: http://doi.org/10.5125/jkaoms.2010.36.2.128
Abstract
- Mesenchymal chondrosarcoma is very aggressive and represents approximately 1% of all chondrosarcomas. While it affects a very wide age range, the peak frequency is in the second decade of life. It may occur in the head and rib region with a predilection for the maxillofacial skeleton. The small cell undifferentiated component may assume a hemangiopericytoma-like vascular pattern and should be distinguished from hemangiopericytoma. Treatment is en bloc resection, the intended tissue margins of excision should be designed to extend well beyond the actual tumor margin, as mesenchymal chondrosarcomas. Aggressive behavior of mesenchymal chondrosarcoma of the jaw, with a tendency for delayed recurrence and metastasis even many years after treatment. The most frequent site of metastasis was the lung. Here we present 52 years old , female case of mesenchymal chondrosarcoma occurs on Rt. mandible.
MeSH Terms
Figure
-

Fig. 1. Gingival swelling and indulation observed on right posterior mandibular area.
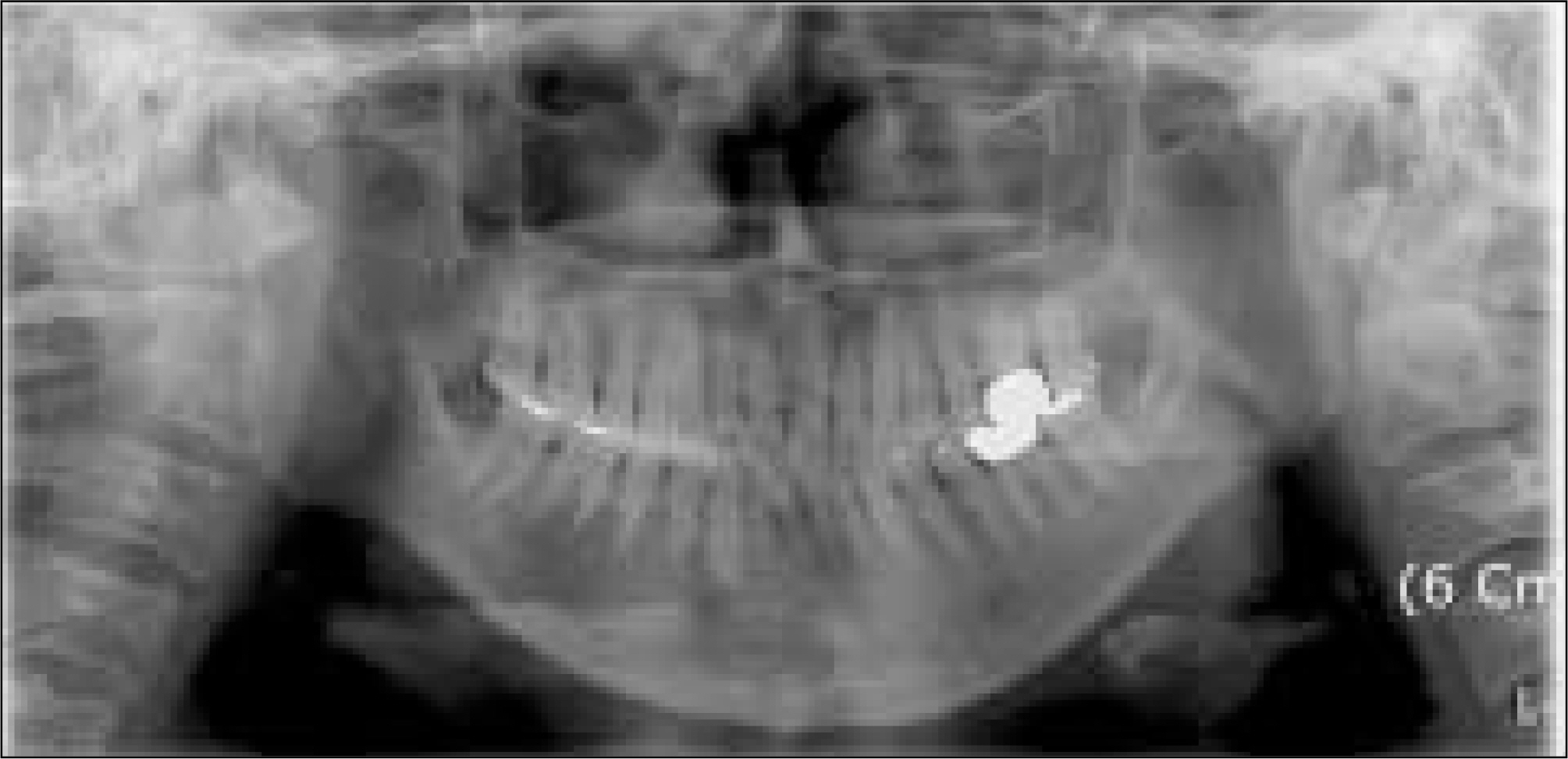
Fig. 2. Panoramic view of 57-years-old showing radiolucent lesion on right mandible and root resorption on involved teeth. Irregular and poor defined margin are observed.

Fig. 3. Section from mandible shows undifferentiated small round cell proliferation with hemangiopericytomatous vascular pattern. Although definite hyaline cartilage island is not seen.(H&E, x100)
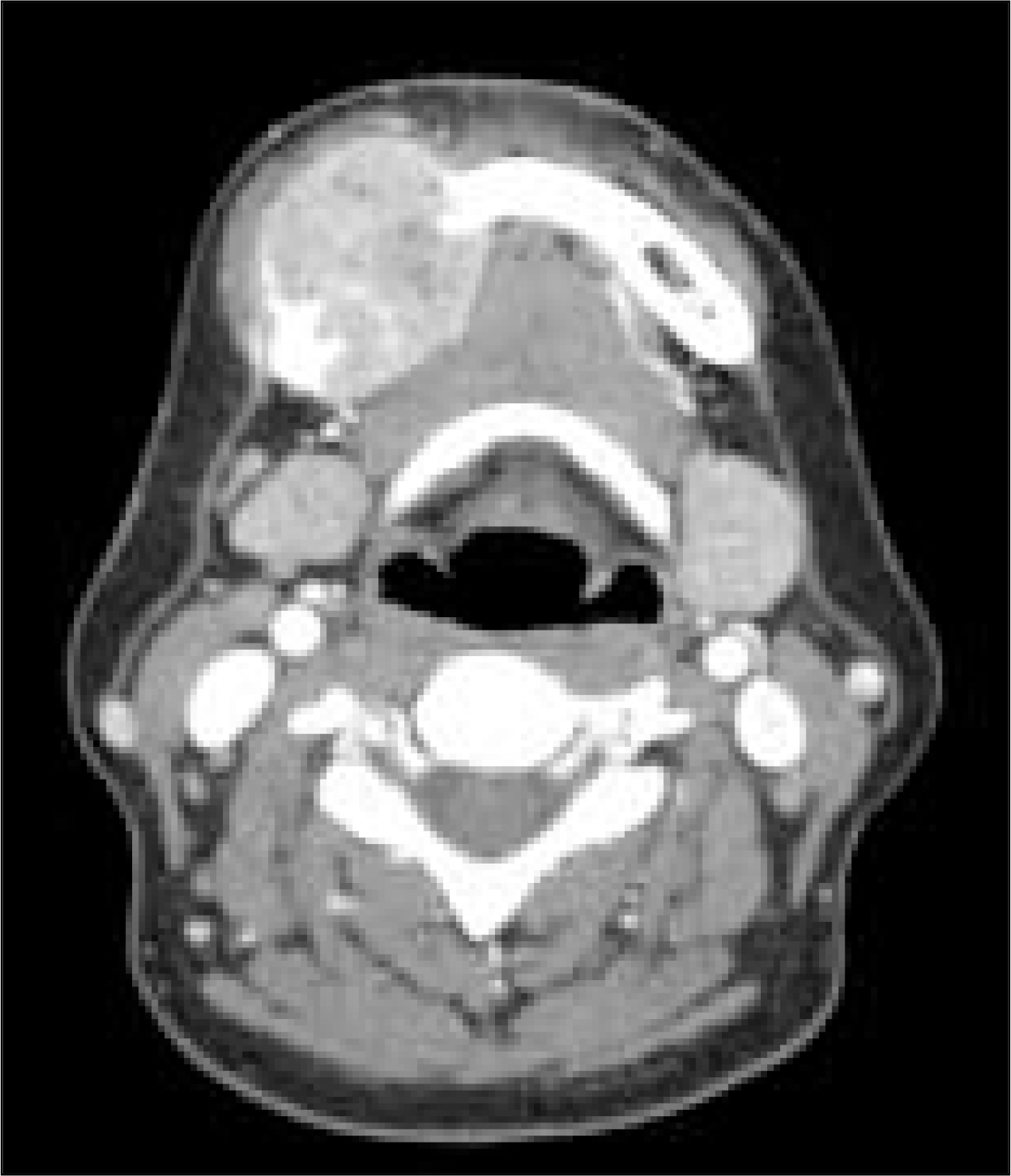
Fig. 4. Preoperative CT. CT shows mass at right mandible body invasion to left sublingual space, mylohyoid muscle and right mandibular buccal space. (CT: computed tomography)

Fig. 5. A slightly imbalanced intake of FDG was found on the right posterior mandibular area. (FDG: fluorodeoxyglucose)
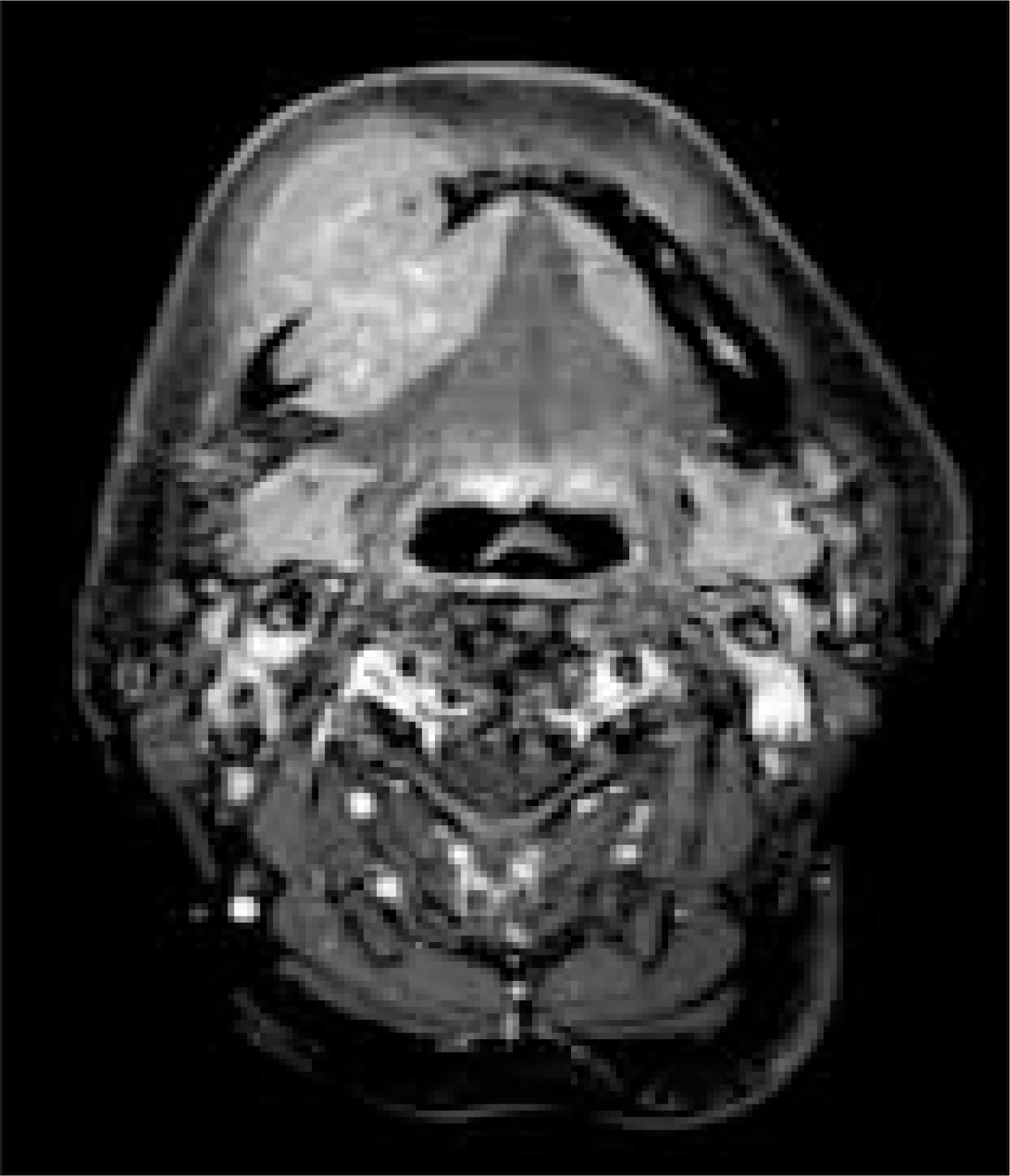
Fig. 6. Preoperative MRI. Highly suggesting malignant mass at right mandible body invasion to right buccal space, right sublingual space, mylohyoid muscle. (T1 weighted image)(MRI: magnetic resonance imaging)

Fig. 7. Postoperative panorama. Reconstruction using by bridging plate & radial forearm flap.

Fig. 8. Mass appears relatively well defined margin and measured about 70×45×35 mm.
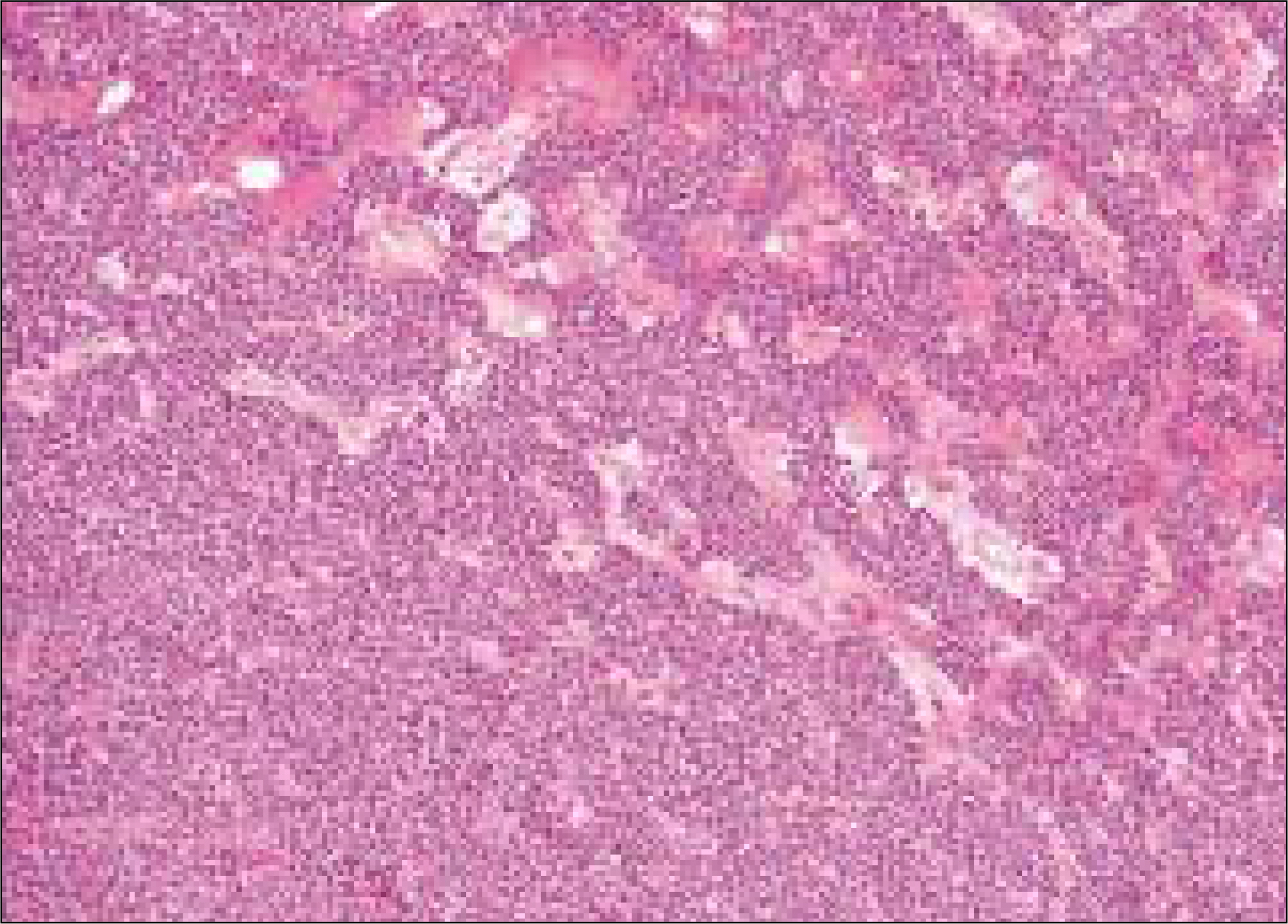
Fig. 9. Section shows mass consisted of undifferentiated small round cell proliferation with hemangiopericytomatous vascular pattern and amorphous chondroid tissue. (H&E, x100)
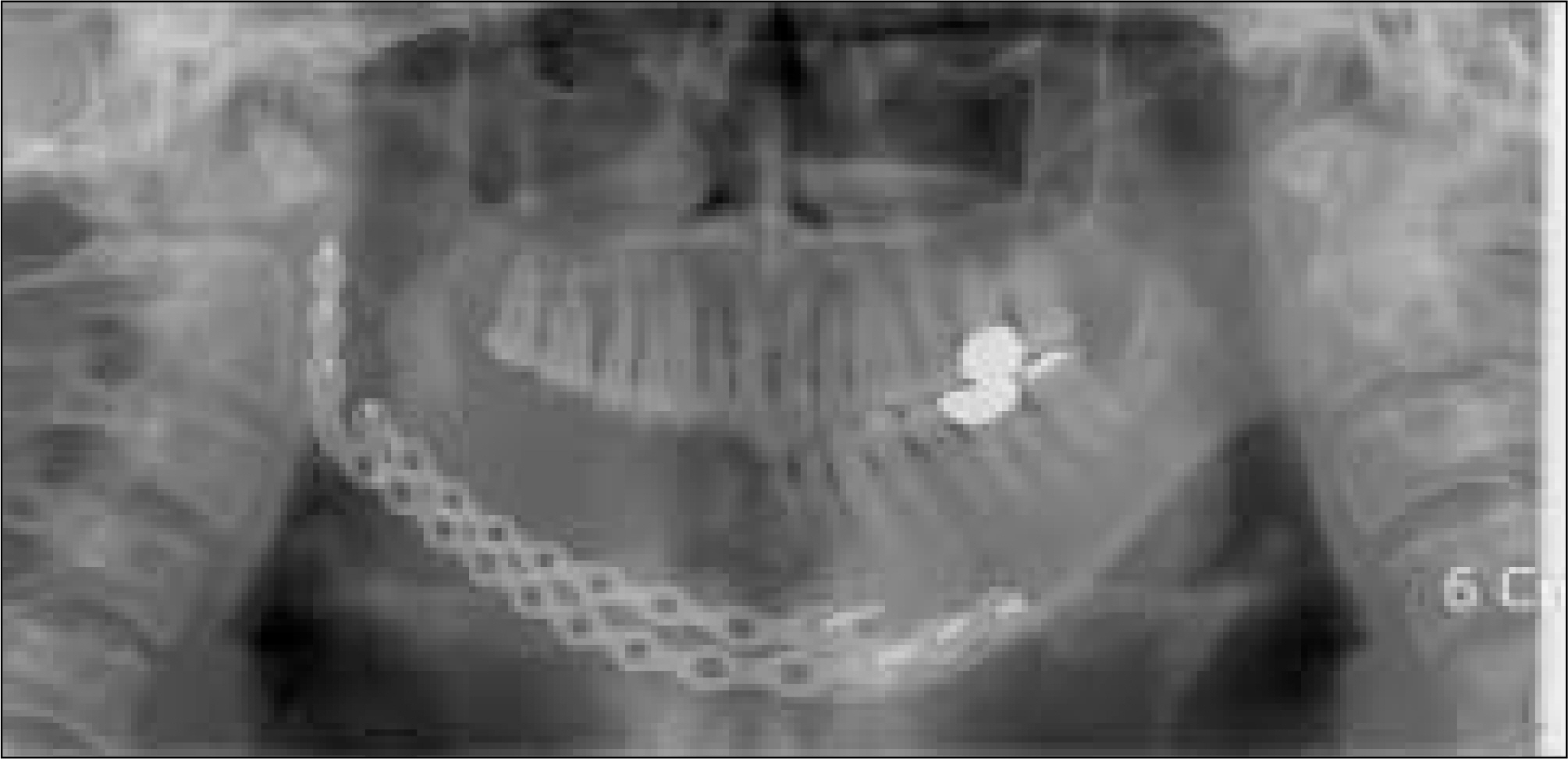
Fig. 10. Panorama shows fracture occurred on reconstructive bridging plate.

Fig. 11. More heavy plate using on secondary surgery.
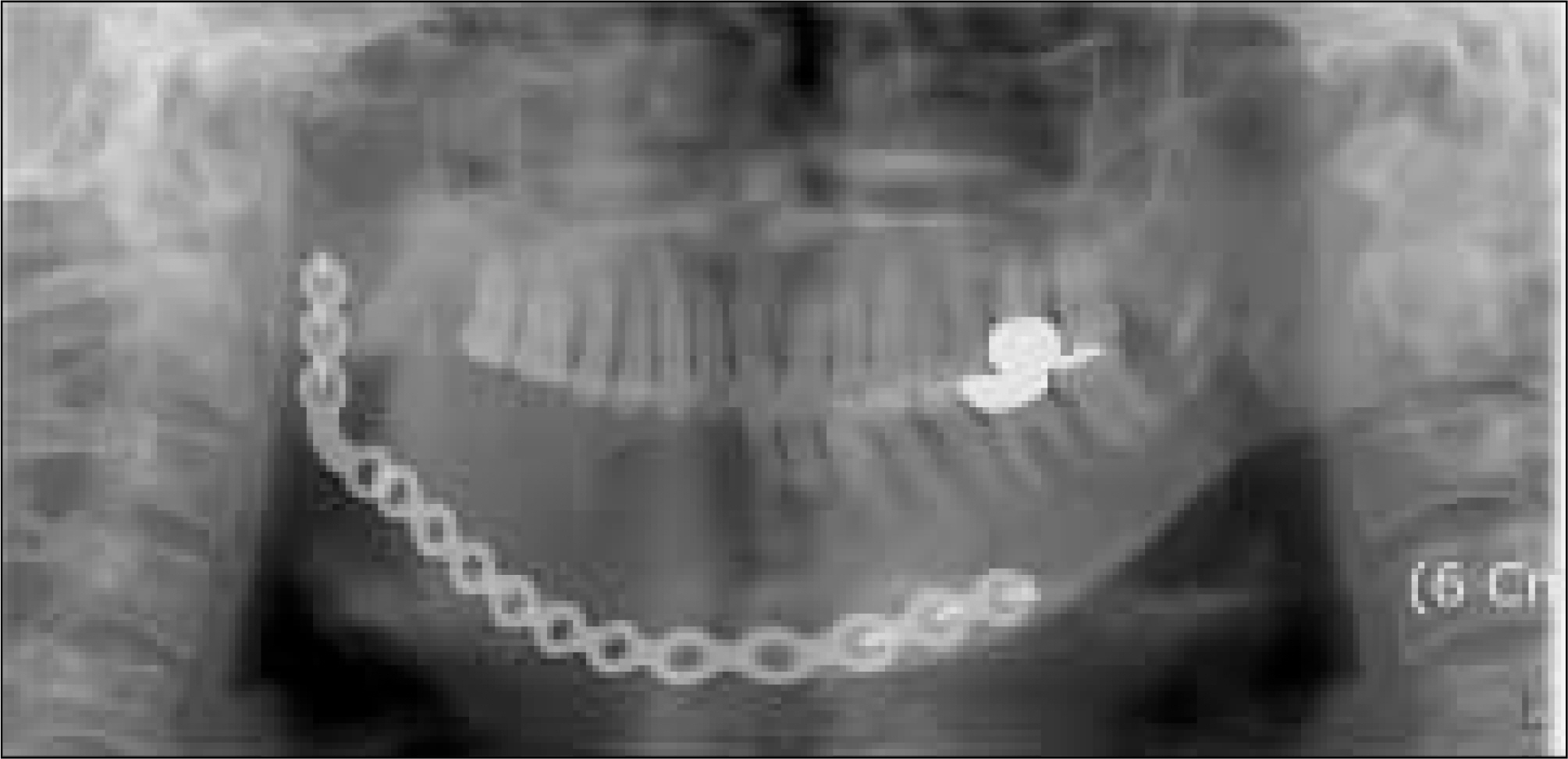
Fig. 12. Fracture occurred the second time.

Fig. 13. Reconstruction using by block bone on iliac crest and reconstruction bridging plate.
Reference
-
References
1. Mu ¨ller S, So ¨der S, Oliveira AM, Inwards CY, Aigner T. Type II collagen as specific marker for mesenchymal chondrosarcomas compared to other small cell sarcomas of the skeleton. Mod Pathol. 2005; 18:1088–94.
Article2. Pellitteri PK, Ferlito A, Fagan JJ, Sua ′ rez C, Devaney KO, Rinaldo A. Mesenchymal chondrosarcoma of the head and neck. Oral Oncol. 2007; 43:970–5.
Article3. Aigner T, Loos S, Mu ¨ller S, Sandell LJ, Unni KK, Kirchner T. Cell differentiation and matrix gene expression in mesenchymal chondrosarcomas. Am J Pathol. 2000; 156:1327–35.
Article4. Aziz SR, Miremadi AR, McCabe JC. Mesenchymal chondrosarcoma of the maxilla with diffuse metastasis: case report and literature review. J Oral Maxillofac Surg. 2002; 60:931–5.
Article5. Crawford JG, Oda D, Egbert M, Myall R. Mesenchymal chondrosarcoma of the maxilla in a child. J Oral Maxillofac Surg. 1995; 53:938–41.
Article6. Zakkak TB, Flynn TR, Boguslaw B, Adamo AK. Mesenchymal chondrosarcoma of the mandible: case report and review of the literature. J Oral Maxillofac Surg. 1998; 56:84–91.
Article7. Dantonello TM, Int-Veen C, Leuschner I, Schuck A, Furtwaengler R, Claviez A, et al. Mesenchymal chondrosarcoma of soft tissues and bone in children, adolescents, and young adults: experiences of the CWS and COSS study groups. Cancer. 2008; 112:2424–31.8. Knott PD, Gannon FH, Thompson LD. Mesenchymal chondrosarcoma of the sinonasal tract: a clinicopathological study of 13 cases with a review of the literature. Laryngoscope. 2003; 113:783–90.
Article9. Christensen RE Jr. Mesenchymal chondrosarcoma of the jaws. Oral Surg Oral Med Oral Pathol. 1982; 54:197–206.
Article10. Ceylan A, Kagan Degerliyurt M, Celenk F, Atac¸ MS, Sabri Uslu S. Haemangiopericytoma of the hard palate. Dentomaxillofac Radiol. 2008; 37:58–61.
Article11. Gadwal SR, Fanburg-Smith JC, Gannon FH, Thompson LD. Primary chondrosarcoma of the head and neck in pediatric patients: a clinicopathologic study of 14 cases with a review of the literature. Cancer. 2000; 88:2181–8.12. Dunfee BL, Sakai O, Pistey R, Gohel A. Radiologic and pathologic characteristics of benign and malignant lesions of the mandible. Radiographics. 2006; 26:1751–68.
Article13. Berk R, Heller A, Heller D, Schwartz S, Klein EA. Ewing's sarcoma of the mandible: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995; 79:159–62.14. Folpe AL, Hill CE, Parham DM, O'Shea PA, Weiss SW. Immunohistochemical detection of FLI-1 protein expression: a study of 132 round cell tumors with emphasis on CD99-positive mimics of Ewing's sarcoma/primitive neuroectodermal tumor. Am J Surg Pathol. 2000; 24:1657–62.15. Acioğlu E, Cansiz H, Mercan H, Dervis¸oğlu S. Head and neck hemangiopericytomas: diagnostic contradictions. J Craniofac Surg. 2009; 20:930–5.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Mesenchymal Chondrosarcoma of the Orbit: A case report and review of the literature
- Mesenchymal Chondrosarcoma Involving Posterior Bone of C7, T1, T2 and Adjacent Muscles
- Mesenchymal Chondrosarcoma: A Case Report
- Extraskeletal Mesenchymal Chondrosarcoma of the Mediastinum: A Case Report
- Mesenchymal Chondrosarcoma: A Case Report
