Measurement of the Weight-bearing Standing Coronal and Sagittal Axial Alignment of Lower Extremity in Young Korean Adults
- Affiliations
-
- 1Department of Orthopedic Surgery, Konkuk University School of Medicine, Seoul, Korea. kwangjun@kuh.ac.kr
- KMID: 2185442
- DOI: http://doi.org/10.4055/jkoa.2011.46.3.191
Abstract
- PURPOSE
The aim of this study was to establish a measurement standard for the weight-bearing axial alignment of the lower extremities when performing a lower extremity reconstruction.
MATERIALS AND METHODS
Among 274 patients (147 males and 127 females) in their 20s to 30s without any physical disabilities, and who had undergone weight-bearing full leg standing radiographs, 188 patients (100 males and 88 females) were examined this study. The data was analyzed further according to their age and gender using the radiographic value on the coronal and sagittal alignment of the lower extremities.
RESULTS
The weight bearing ratio was 38.47+/-10.52% on the coronal plane and 36.11+/-7.88% on the sagittal plane. Both the mechanical axis and the the weight bearing axis were not identical due to their 0.68+/-0.89degrees difference on average. The most adjacent point of the femoral condyles to the tibial plateau on the sagittal plane was assigned to the center of the knee joint. The difference between the mechanical axis and weight bearing axis was 0.04degrees, which was not significant.
CONCLUSION
There is a difference between the mechanical axis, which consists of both a line from the center of the femoral head to the center of knee joint and a line from the center of the knee joint to the center of ankle joint, and the weight bearing axis, which is linked directly from the center of the femoral head to the center of the ankle joint. Furthermore, the weight bearing axis passes through the anteromedial part in the knee joint. The center of the knee joint is defined as the most adjacent point of both femoral condyle to the tibial plateau on the sagittal plane.
Keyword
MeSH Terms
Figure
-

Figure 1 Weight bearing full leg standing view. (A) About 1/2-1/3 of fibular head Overlaps with tibial condyle in anteroposterior view. (B) Lateral view. Both femoral condyles overlap each other. (C) Antero-posterior view position. Spreading legs as the width between both femoral head center and patella forward facing. (D) Lateral view position. One leg standing weight bearing position.
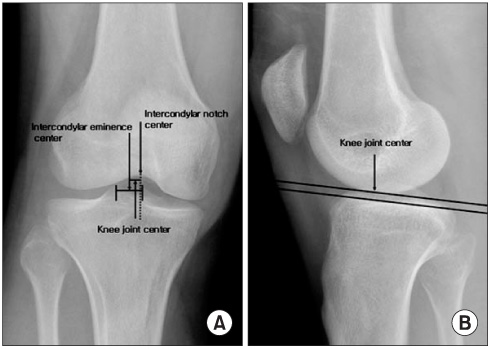
Figure 2 Knee joint center. (A) Points used to determine the center of the knee in coronal plane are shown. (B) Points used to determine the center of the knee in sagittal plane are shown.
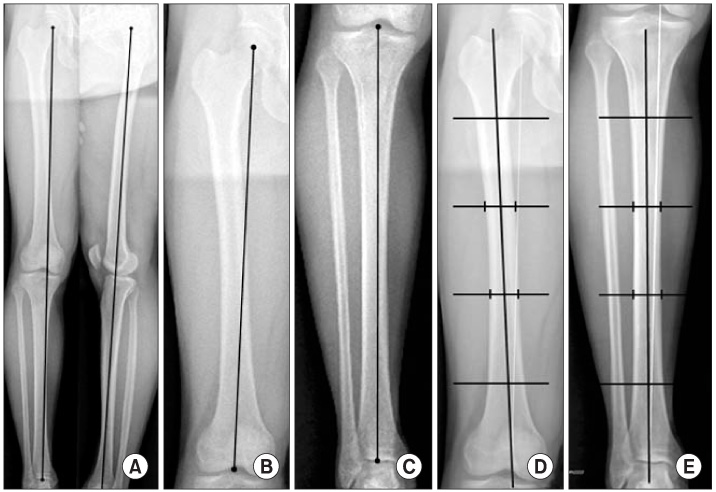
Figure 3 Weight-bearing axis (A), femoral mechanical axis (B), tibial mechanical axis, (C), femoral anatomical axis (D) and tibial anatomical axis (E) are shown.

Figure 4 Weight-bearing ratio. (A) In coronal plane view, weight bearing ratio is (a/b)×100. (B) In sagittal plane view, femur weight bearing ratio is {a/(a+b)}×100, and tibia weight bearing ratio is {c/(c+d)}×100.

Figure 5 Various angles in coronal plane view are shown. (A) femoro-tibial anatomical angle, (B) angle of femoral anatomical axis-weight bearing axis, (C) angle of tibial anatomical axis-weight bearing axis, angle, (D) angle of femoral mechanical axis-weight bearing axis, (E) angle of tibial mechanical axis-weight bearing axis, (F) femoral bowing angle, (G) tibial bowing angle.
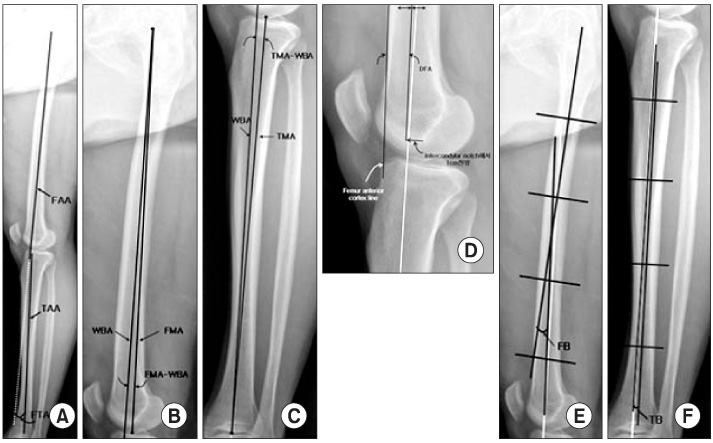
Figure 6 Various angles in coronal plane view are shown. (A) femoro-tibial anatomical angle, (B) angle of femoral mechanical axis-weight bearing axis, (C) angle of tibial mechanical axis-weight bearing axis, (D) distal femoral anterior angle, (E) femoral bowing angle, (F) tibial bowing angle.

Figure 7 On sagittal plane view, tibial posterior slope angle for weight bearing axis (α), for anterior tibial cortex (β), for fibular shaft (γ), and for tibial anatomical axis (δ) are drawn.
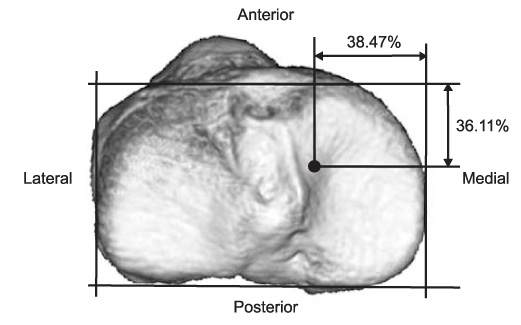
Figure 8 Diagram showing the point on the tibial plateau through which the weight bearing axis passes.

Figure 9 Scatter diagram of the weight bearing ratio points.
Reference
-
1. Moreland JR. Mechanisms of failure in total knee arthroplasty. Clin Orthop Relat Res. 1988. (226):49–64.
Article2. Canale ST, Beaty JH. Campbell's operative orthopaedics. 2008. 11th ed. Philadelphia: Mosby Inc;249–250.3. Tang WM, Zhu YH, Chiu KY. Axial alignment of the lower extremity in Chinese adults. J Bone Joint Surg Am. 2000. (11):1603–1608.
Article4. Chung BJ, Kang YG, Chang CB, Kim SJ, Kim TK. Differences between sagittal femoral mechanical and distal reference axes should be considered in navigated TKA. Clin Orthop Relat Res. 2009. 467:2403–2413.
Article5. Han HS, Chang CB, Seong SC, Lee S, Lee MC. Evaluation of anatomic references for tibial sagittal alignment in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2008. 16:373–377.
Article6. Seo JG, Kim BK, Moon YW, et al. Bony landmarks for determining the mechanical axis of the femur in the sagittal plane during total knee arthroplasty. Clin Orthop Surg. 2009. 1:128–131.
Article7. Minoda Y, Kobayashi A, Iwaki H, et al. Sagittal alignment of the lower extremity while standing in Japanese male. Arch Orthop Trauma Surg. 2008. 128:435–442.
Article8. Sugama R, Minoda Y, Kobayashi A, et al. Sagittal alignment of the lower extremity while standing in female. Knee Surg Sports Traumatol Arthrosc. 2011. 19:74–79.
Article9. Ahlbäck S. Osteoarthrosis of the knee. A radiographic investigation. Acta Radiol Diagn (Stockh). 1968. Suppl 277. 7–72.10. Hernborg JS, Nilsson BE. The natural course of untreated osteoarthritis of the knee. Clin Orthop Relat Res. 1977. (123):130–137.
Article11. White SH, Ludkowski PF, Goodfellow JW. Anteromedial osteoarthritis of the knee. J Bone Joint Surg Br. 1991. 73:582–586.
Article12. Johnson F, Leitl S, Waugh W. The distribution of load across the knee: a comparison of static and dynamic measurements. J Bone Joint Surg Br. 1980. 62:346–349.
Article13. Ahn TJ, Kim JK, Ahn BW, Park CH. Standardization of preoperative radiography for total knee arthroplasty. J Korean Knee Soc. 1994. 6:158–164.14. Moreland JR, Bassett LW, Hanker GJ. Radiographic analysis of the axial alignment of the lower extremity. J Bone Joint Surg Am. 1987. 69:745–749.
Article15. Tew M, Waugh W. Tibiofemoral alignment and the results of knee replacement. J Bone Joint Surg Br. 1985. 67:551–556.
Article16. Hsu RW, Himeno S, Coventry MB, Chao EY. Normal axial alignment of the lower extremity and load-bearing distribution at the knee. Clin Orthop Relat Res. 1990. (255):215–227.
Article17. Oswald MH, Jakob RP, Schneider E, Hoogewoud HM. Radiological analysis of normal axial alignment of femur and tibia in view of total knee arthroplasty. J Arthroplasty. 1993. 8:419–426.
Article18. Karakaş HM, Harma A. Femoral shaft bowing with age: a digital radiological study of Anatolian Caucasian adults. Diagn Interv Radiol. 2008. 14:29–32.19. Yehyawi TM, Callaghan JJ, Pedersen DR, O'Rourke MR, Liu SS. Variances in sagittal femoral shaft bowing in patients undergoing TKA. Clin Orthop Relat Res. 2007. 464:99–104.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Weight Bearing Study Using Digital Scales in Hemiplegic Patients
- The Appearance and the Axial Alignment of the Lower Extremity
- The Effect of Sagittal Knee Deformity on Preoperative Measurement of Coronal Mechanical Alignment during Total Knee Arthroplasty
- Knee Extension Is Related to the Posteriorly Deviated Gravity Line to the Pelvis in Young Adults: Radiographic Analysis Using Low-Dose Biplanar X-ray
- Sagittal Parameters of Spine and Pelvis in Young Adults Using the EOS Imaging System: Prospective Study of 92 Asymptomatic Subjects
