Single Bone Fixation with Flexible Intramedullary Nail for Displaced Both Forearm Bone Shaft Fractures in Children
- Affiliations
-
- 1Department of Orthopaedic Surgery, Ewha Womans University College of Medicine, Seoul, Korea. wwiiw@hanmail.net
- KMID: 2185320
- DOI: http://doi.org/10.4055/jkoa.2012.47.5.360
Abstract
- PURPOSE
In the present study, the usefulness of single bone flexible intramedullary nail fixation in pediatric displaced both forearm bone shaft fractures was evaluated.
MATERIALS AND METHODS
From 2006, we treated 14 consecutive pediatric both forearm bone shaft fractures using a single bone flexible intramedullary fixation. The average age of patients was 8.6 years (range, 3-12 years). We nailed the one bone of the two that showed either greater deformity in the initial radiographs, or difficulty in maintaining reduction, which in our cases was usually the radius. The operation time, duration of cast removal, functional recovery and complications were evaluated. The bony alignment, maintained until bony union, was analyzed by radiographic assessment. These data were compared with 27 cases of both bone nailing, which was the standard treatment in our institution prior to 2006.
RESULTS
All cases in both groups healed without secondary intervention. All cases recovered to a normal functional status after postoperative average 12 weeks. In regards to their clinical and radiographic results, there was no significant difference between the single bone fixation group and the both bone fixation group, except that there was a shorter operation time, and longer period of cast immobilization, for the single bone fixation group.
CONCLUSION
Single bone flexible intramedullary fixation is a useful method for the treatment of displaced forearm bone shaft fractures in children. The strategy of fixating the bone that exhibits greater deformity or difficulty in maintaining reduction, which was usually the radius, was found to be effective in our cases.
Keyword
Figure
-
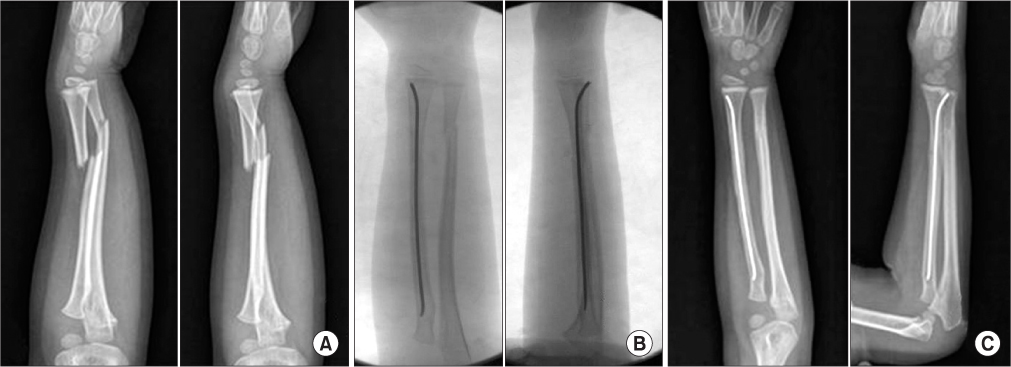
Figure 1 Fixation principle I: The more displaced bone was fixated. (A) Preoperative radiograph of a 12-year-old girl shows the radius was more displaced. (B) Intraoperative fluoroscopy shows the radius was fixated, as it was more displaced. The alignment of the ulnar and its stability were maintained after single bone intramedullary fixation of the radius. (C) Final radiograph shows the alignment of both forearm bones was well maintained until bony union was achieved.
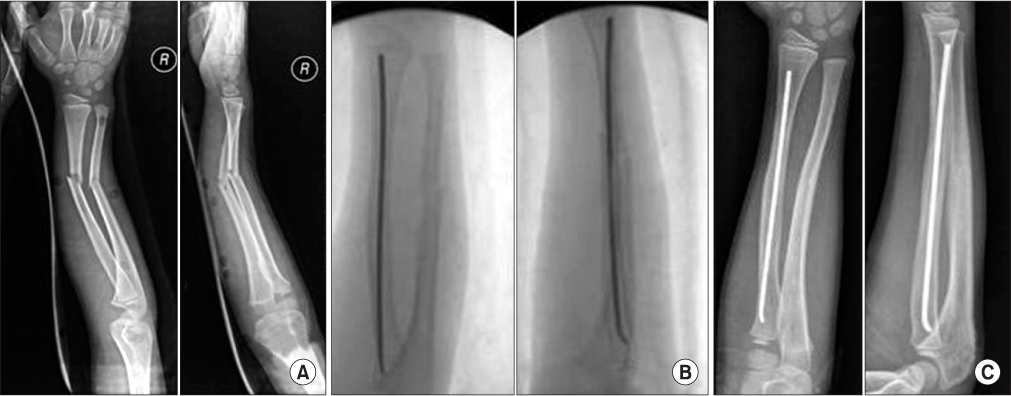
Figure 2 Fixation principle II: The bone more difficult to reduce or control was fixated. (A) Preoperative radiograph of a 8-year-old boy shows both bones were equally displaced. (B) Intraoperative fluoroscopy shows the radius was fixated, as the radius was usually more difficult to reduce and maintain its reduction. The alignment of the ulna and its stability were maintained after single bone intramedullary fixation of the radius. (C) Radiograph shows the alignment of both forearm bones was well maintained until bony union was achieved.

Figure 3 A complication occurring in single bone intramedullary fixation. (A) Radiograph was taken just before nail removal at postoperative 13 months. (B) A fracture developed at the entry site of the nail during the difficult procedure of nail removal.
Reference
-
1. Benson M, Fixsen J, Macnicol M, Parsch K. Children's orthopaedics & fractures. 2002. 2nd ed. New York: Churchill Livingstone;609–632.2. Flynn JM, Waters PM. Single-bone fixation of both-bone forearm fractures. J Pediatr Orthop. 1996. 16:655–659.
Article3. Shoemaker SD, Comstock CP, Mubarak SJ, Wenger DR, Chambers HG. Intramedullary Kirschner wire fixation of open or unstable forearm fractures in children. J Pediatr Orthop. 1999. 19:329–337.
Article4. Myers GJ, Gibbons PJ, Glithero PR. Nancy nailing of diaphyseal forearm fractures. Single bone fixation for fractures of both bones. J Bone Joint Surg Br. 2004. 86:581–584.5. Houshian S, Bajaj SK. Forearm fractures in children. Single bone fixation with elastic stable intramedullary nailing in 20 cases. Injury. 2005. 36:1421–1426.
Article6. Dietz JF, Bae DS, Reiff E, Zurakowski D, Waters PM. Single bone intramedullary fixation of the ulna in pediatric both bone forearm fractures: analysis of short-term clinical and radiographic results. J Pediatr Orthop. 2010. 30:420–424.
Article7. Kirkos JM, Beslikas T, Kapras EA, Papavasiliou VA. Surgical treatment of unstable diaphyseal both-bone forearm fractures in children with single fixation of the radius. Injury. 2000. 31:591–596.
Article8. Lascombes P, Prevot J, Ligier JN, Metaizeau JP, Poncelet T. Elastic stable intramedullary nailing in forearm shaft fractures in children: 85 cases. J Pediatr Orthop. 1990. 10:167–171.
Article9. Verstreken L, Delronge G, Lamoureux J. Shaft forearm fractures in children: intramedullary nailing with immediate motion: a preliminary report. J Pediatr Orthop. 1988. 8:450–453.10. Fuller DJ, McCullough CJ. Malunited fractures of the forearm in children. J Bone Joint Surg Br. 1982. 64:364–367.
Article11. Blount WP. Forearm fractures in children. Clin Orthop Relat Res. 1967. 51:93–107.
Article12. Hunter JB. The principles of elastic stable intramedullary nailing in children. Injury. 2005. 36:Suppl 1. A20–A24.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pediatric Forearm Bone Fractures Treated with Flexible Intramedullary Nail
- Operative Treatment in Fractures of the Humeral Shaft: Comparison of the Clinical Results of Flexible Intramedullary Nailing Versus Interlocking Intramedullary Nailing
- Flexible Intramedullary Nail Fixation of Pediatric Femoral Shaft Fracture
- Retrieval of a Broken Intramedullary Nail after Refracture of Femoral Shaft: A case report
- Interlocking Intramedullary Nailing of Forearm Shaft Fractures in Adults
