CT Colonography
- Affiliations
-
- 1Department of Radiology, Seoul National University College of Medicine, Korea. shkim@radcom.snu.ac.kr
- KMID: 2184793
- DOI: http://doi.org/10.5124/jkma.2007.50.1.33
Abstract
- CT colonography is a recent radiologic technique enabling detection of tumoral lesions in the colon. Since double contrast barium enema has lost most of its adherents, CT colonography gives a great opportunity for radiologists to play a predominant role in the diagnosis and treatment of colorectal cancer and adenoma. CT colonography has dramatically evolved by the refinement of the existing techniques and the introduction of new techniques such as fecal tagging, the use of carbon dioxide to inflate the colon, multi-detector row CT scanners, the use of ultra-low dose scan protocols, and computer-aided detection. These technical improvements are helpful both to the radiologists and to the patients. Several technical factors should be considered for the successful performance of CT colonography. Fecal tagging improves patients' compliance by allowing for reduced bowel preparation. It facilitates the differentiation of true polyp from residual feces, resulting in the improvement of diagnostic accuracy. Automated carbon dioxide insufflation is more efficient and safer in colonic distention compared to manual room air insufflation. CT colonography should be performed by using a thin collimation of < or =3mm with a reconstruction increment of < or =3 mm and a low radiation dose of 30mAs to 50mAs. There are two strategies to interpret CT colonography dataset; primary 2D and 3D interpretation. There is not a single correct method for interpretation of CTC; therefore, the radiologists should be well-versed with both methods of interpretation. Finally, radiologists should also be familiar with potential diagnostic pitfalls, false positive and false negative findings. In experienced hands, CT colonography seems to be ripe for prime-time colorectal cancer screening. However, it is not yet ready for widespread application of screening due to various drawbacks. Therefore, considerable efforts should be undertaken to take it to the level of being a widely accepted screening method for colorectal cancer.
MeSH Terms
Figure
-

Figure 1 Fecal tagging using 40% high concentration of barium (A) Stool tagging. Solid stools (arrows) are tagged homogeneously and appear white (B) Fluid tagging. Residual fluid (arrow) in distal transverse colon is tagged homogeneously and appears white

Figure 2 CT colonography using 3D virtual colon dissection technique. 3D virtual colon dissection technique was developed to inspect the inner colonic surface by virtually dissecting the colon along its longitudinal axis. A 6mm sessile polyp (arrow) is seen in the sigmoid colon
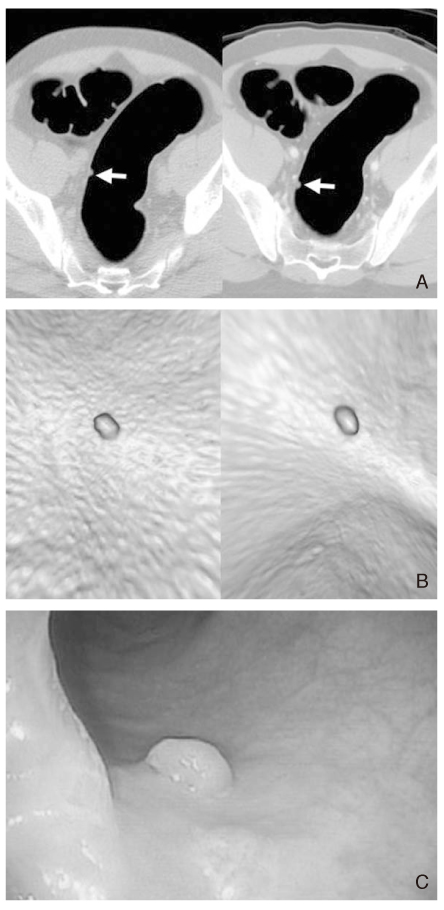
Figure 3 A 6mm sessile polyp (A) 2D axial CT images. In both supine (left) and prone (right) positions, a sessile polypoid lesion (arrows) having homogeneous soft tissue attenuation is seen without position change in the sigmoid colon (B) 3D endoluminal images. A polyp shows same shape in both supine (left) and prone (right) positions (C) Conventional colonoscopic image. This lesion was confirmed as a low grade tubular adenoma on pathologic examination
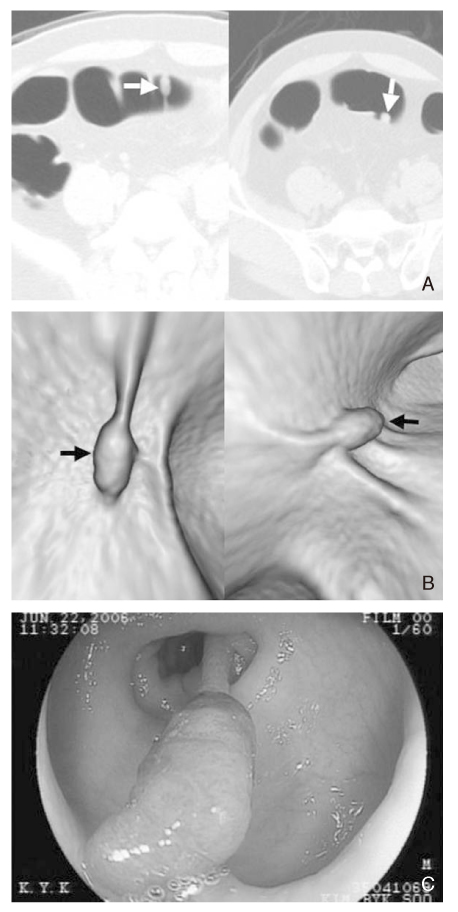
Figure 4 A 1cm pedunculated polyp (A, B) 2D axial (A) and 3D endoluminal (B) images. Images in a prone position (left) show a pedunculated polyp (arrow) having a long stalk. The lesion shows collapsed shape on supine images (right) (C) Conventional colonoscopic image. This lesion was confirmed as a low grade tubular adenoma on pathologic examination

Figure 5 Normal ileocecal valve (A) On 3D endoluminal image, a polypoid mass-like lesion (arrow) is shown (B) On 2D axial image with soft tissue window, this (arrow) stands in a characteristic location and possesses homogeneous fatty internal attenuation, indicating ileocecal valve

Figure 6 Diverticula in the ascending colon (A) 3D endoluminal image shows two diverticular orifices (arrows) projecting from the colonic lumen at the area just proximal to the ileocecal valve (*) (B) 2D axial CT scan shows focal outpouchings (arrows) of the colonic lumen

Figure 7 Impacted diverticulum (A) 3D endoluminal image demonstrates a polypoid filling defect (arrow) which is protruded into the colonic lumen (B) 2D axial CT image with soft tissue window shows the filling defect (arrow) to project beyond the colonic wall into the pericolic fat and contain barium and air, indicating the defect is retained stool and barium within a diverticulum

Figure 8 Colon cancer (A) On 3D endoluminal image, an irregularly flat and elevated lesion (arrow) is seen (B) This lesion (arrow) appears an eccentric wall thickening of the colon on 2D axial CT image (C) Colonoscopic image demonstrates similar appearance to that of 3D endoluminal image. This lesion was diagnosed as a colon cancer after right hemicolectomy

Figure 9 Occlusive colon cancer (A) 3D endoluminal image depicts a large and irregular mass (arrow) with luminal narrowing (B) 3D transparency view shows classic apple-core lesion (arrow) in the sigmoid colon (C) On 2D axial, enhanced CT image, segmental wall thickening (arrow) with abnormal enhancement is seen, indicating sigmoid colon cancer. Note pericolic fat stranding and small lymph nodes around colonic mass. The findings on 2D images enable us to determine local staging of colorectal cancer
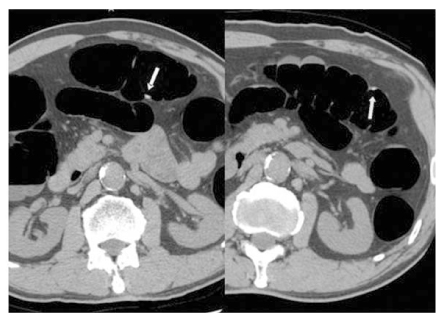
Figure 10 Feces showing position change. Image in a supine position (left) shows a small polypoid lesion (arrow) in the transverse colon. In a prone position (right), this lesion (arrow) moved to a dependent portion of the colon, indicating feces
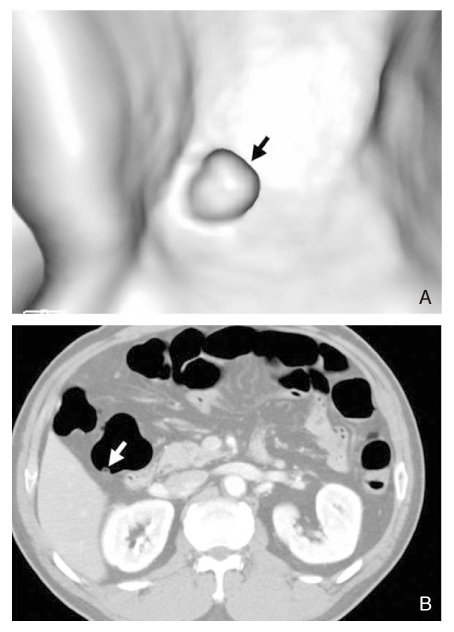
Figure 11 Feces containing air (A) On 3D endoluminal view, a polypoid lesion (arrow) projecting into the colonic lumen is seen (B) On 2D axial image with soft tissue window, the lesion (arrow) has typical feature of feces, that is, central pockets of air

Figure 12 Feces with angular margin. 3D endoluminal images demonstrate angular margins of feces (arrows). On the contrary, true polyps show round, oval, or lobulating contour (not shown)
Reference
-
1. Vining DJ, Gelfand DW, Bechtold RE. Technical feasibility of colon imaging with helical CT and virtual reality. AJR Am J Roentgenol. 1994. 162:104.2. Fenlon HM, Nunes DP, Schroy PC 3rd, Barish MA, Clarke PD, Ferrucci JT. A comparison of virtual and conventional colonoscopy for the detection of colorectal polyps. N Engl J Med. 1999. 341:1496–1503.
Article3. Pickhardt PJ, Choi JR, Hwang I, Butler JA, Puckett ML, Hildebrandt HA, Wong RK, Nugent PA, Mysliwiec PA, Schindler WR. Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. N Engl J Med. 2003. 349:2191–2200.
Article4. Rockey DC, Paulson E, Niedzwiecki D, Davis W, Bosworth HB, Sanders L, Yee J, Henderson J, Hatten P, Burdick S, Sanyal A, Rubin DT, Sterling M, Akerkar G, Bhutani MS, Binmoeller K, Garvie J, Bini EJ, McQuaid K, Foster WL, Thompson WM, Dachman A, Halvorsen R. Analysis of air contrast barium enema, computed tomographic colonography, and colonoscopy: prospective comparison. Lancet. 2005. 365:305–311.
Article5. Cotton PB, Durkalski VL, Pineau BC, Palesch YY, Mauldin PD, Hoffman B, Vining DJ, Small WC, Affronti J, Rex D, Kopecky KK, Ackerman S, Burdick JS, Brewington C, Turner MA, Zfass A, Wright AR, Iyer RB, Lynch P, Sivak MV, Butler H. Computed tomographic colonography (virtual colonoscopy): a multicenter comparison with standard colonoscopy for detection of colorectal neoplasia. JAMA. 2004. 291:1713–1719.
Article6. Mulhall BP, Veerappan GR, Jackson JL. Meta-analysis: computed tomographic colonography. Ann Intern Med. 2005. 142:635–650.
Article7. O'Brien MJ, Winawer SJ, Zauber AG, Gottlieb LS, Sternberg SS, Diaz B, Dickersin GR, Ewing S, Geller S, Kasimian D, et al. The National Polyp Study. Patient and polyp characteristics associated with high-grade dysplasia in colorectal adenomas. Gastroenterology. 1990. 98:371–379.8. Winawer SJ, Zauber AG. The advanced adenoma as the primary target of screening. Gastrointest Endosc Clin N Am. 2002. 12:1–9.
Article9. Anderson WF, Guyton KZ, Hiatt RA, Vernon SW, Levin B, Hawk E. Colorectal cancer screening for persons at average risk. J Natl Cancer Inst. 2002. 94:1126–1133.
Article10. Winawer SJ, Fletcher RH, Miller L, Godlee F, Stolar MH, Mulrow CD, Woolf SH, Glick SN, Ganiats TG, Bond JH, Rosen L, Zapka JG, Olsen SJ, Giardiello FM, Sisk JE, Van Antwerp R, Brown-Davis C, Marciniak DA, Mayer RJ. Colorectal cancer screening: clinical guidelines and rationale. Gastroenterology. 1997. 112:594–642.
Article11. Rex DK, Cutler CS, Lemmel GT, Rahmani EY, Clark DW, Helper DJ, Lehman GA, Mark DG. Colonoscopic miss rates of adenomas determined by back-to-back colonoscopies. Gastroenterology. 1997. 112:292–294.
Article12. Bressler B, Paszat LF, Vinden C, Li C, He J, Rabeneck L. Colonoscopic miss rates for right-sided colon cancer: a population-based analysis. Gastroenterology. 2004. 127:452–456.
Article13. Leaper M, Johnston MJ, Barclay M, Dobbs BR, Frizelle FA. Reasons for failure to diagnose colorectal carcinoma at colonoscopy. Endoscopy. 2004. 36:499–503.
Article14. Zubarik R, Fleischer DE, Mastropietro C, Lopez J, Carroll J, Benjamin S, Eisen G. Prospective analysis of complications 30 days after outpatient colonoscopy. Gastrointest Endosc. 1999. 50:322–328.
Article15. Morrin MM, Farrell RJ, Kruskal JB, Reynolds K, McGee JB, Raptopoulos V. Utility of intravenously administered contrast material at CT colonography. Radiology. 2000. 217:765–771.
Article16. Johnson CD, MacCarty RL, Welch TJ, Wilson LA, Harmsen WS, Ilstrup DM, Ahlquist DA. Comparison of the relative sensitivity of CT colonography and double-contrast barium enema for screen detection of colorectal polyps. Clin Gastroenterol Hepatol. 2004. 2:314–321.
Article17. Fenlon HM, McAneny DB, Nunes DP, Clarke PD, Ferrucci JT. Occlusive colon carcinoma: virtual colonoscopy in the preoperative evaluation of the proximal colon. Radiology. 1999. 210:423–428.
Article18. Fukutomi Y, Moriwaki H, Nagase S, Tajika M, Naito T, Miwa Y, Yamada Y, Araki H, Okuno M, Nagura K, Kato T, Ninomiya M. Metachronous colon tumors: risk factors and rationale for the surveillance colonoscopy after initial polypectomy. J Cancer Res Clin Oncol. 2002. 128:569–574.
Article19. Gollub MJ, Ginsberg MS, Cooper C, Thaler HT. Quality of virtual colonoscopy in patients who have undergone radiation therapy or surgery: how successful are we? AJR. 2002. 178:1109–1116.
Article20. Laghi A, Iannaccone R, Bria E, Carbone I, Trasatti L, Piacentini F, Lauro S, Vecchione A, Passariello R. Contrast-enhanced computed tomographic colonography in the follow-up of colorectal cancer patients: a feasibility study. Eur Radiol. 2003. 13:883–889.
Article21. Macari M, Berman P, Dicker M, Milano A, Megibow AJ. Usefulness of CT colonography in patients with incomplete colonoscopy. AJR. 1999. 173:561–564.
Article22. Iannaccone R, Catalano C, Mangiapane F, Murakami T, Lamazza A, Fiori E, Schillaci A, Marin D, Nofroni I, Hori M, Passariello R. Colorectal polyps: detection with low-dose multi-detector row helical CT colonography versus two sequential colonoscopies. Radiology. 2005. 237:927–937.
Article23. Macari M, Lavelle M, Pedrosa I, Milano A, Dicker M, Megibow AJ, Xue X. Effect of different bowel preparations on residual fluid at CT colonography. Radiology. 2001. 218:274–277.
Article24. Ehrenpreis ED, Nogueras JJ, Botoman VA, Bonner GF, Zaitman D, Secrest KM. Serum electrolyte abnormalities secondary to Fleet's Phospho-Soda colonoscopy prep. A review of three cases. Surg Endosc. 1996. 10:1022–1024.
Article25. Oliveira L, Wexner SD, Daniel N, DeMarta D, Weiss EG, Nogueras JJ, Bernstein M. Mechanical bowel preparation for elective colorectal surgery. A prospective, randomized, surgeon-blinded trial comparing sodium phosphate and polyethylene glycol-based oral lavage solutions. Dis Colon Rectum. 1997. 40:585–591.
Article26. Ginnerup Pedersen B, Moller Christiansen TE, Viborg Mortensen F, Christensen H, Laurberg S. Bowel cleansing methods prior to CT colonography. Acta Radiol. 2002. 43:306–311.27. Kim SH, Choi BI, Han JK. CT colonography in a Korean population with a high residue diet: comparison between wet and dry preparations. Clin Radiol. 2006. 61:483–494.
Article28. Lefere PA, Gryspeerdt SS, Dewyspelaere J, Baekelandt M, Van Holsbeeck BG. Dietary fecal tagging as a cleansing method before CT colonography: initial results polyp detection and patient acceptance. Radiology. 2002. 224:393–403.
Article29. Lefere P, Gryspeerdt S, Baekelandt M, Van Holsbeeck B. Laxative-free CT colonography. AJR. 2004. 183:945–948.
Article30. Lefere P, Gryspeerdt S, Marrannes J, Baekelandt M, Van Holsbeeck B. CT colonography after fecal tagging with a reduced cathartic cleansing and a reduced volume of barium. AJR. 2005. 184:1836–1842.
Article31. Iannaccone R, Laghi A, Catalano C, Mangiapane F, Lamazza A, Schillaci A, Sinibaldi G, Murakami T, Sammartino P, Hori M, Piacentini F, Nofroni I, Stipa V, Passariello R. Computed tomographic colonography without cathartic preparation for the detection of colorectal polyps. Gastroenterology. 2004. 127:1300–1311.
Article32. Yee J, Hung RK, Akerkar GA, Wall SD. The usefulness of glucagon hydrochloride for colonic distention in CT colonography. AJR. 1999. 173:169–172.
Article33. Morrin MM, Farrell RJ, Keogan MT, Kruskal JB, Yam CS, Raptopoulos V. CT colonography: colonic distention improved by dual positioning but not intravenous glucagons. Eur Radiol. 2002. 12:525–530.
Article34. Taylor SA, Halligan S, Goh V, Morley S, Bassett P, Atkin W, Bartram CI. Optimizing colonic distention for multi-detector row CT colonography: effect of hyoscine butylbromide and rectal balloon catheter. Radiology. 2003. 229:99–108.
Article35. Park SH, Ha HK, Kim MJ, Kim KW, Kim AY, Yang DH, Lee MG, Kim PN, Shin YM, Yang SK, Myung SJ, Min YI. False-negative results at multi-detector row CT colonography: multivariate analysis of causes for missed lesions. Radiology. 2005. 235:495–502.
Article36. Shinners TJ, Pickhardt PJ, Taylor AJ, Jones DA, Olsen CH. Patient-controlled room air insufflation versus automated carbon dioxide delivery for CT colonography. AJR. 2006. 186:1491–1496.
Article37. Pickhardt PJ. Incidence of colonic perforation at CT colonography: review of existing data and implications for screening of asymptomatic adults. Radiology. 2006. 239:313–316.
Article38. Yee J, Kumar NN, Hung RK, Akerkar GA, Kumar PR, Wall SD. Comparison of supine and prone scanning separately and in combination at CT colonography. Radiology. 2003. 226:653–661.
Article39. Fletcher JG, Johnson CD, Welch TJ. Optimization of CT colonography technique: prospective trial in 180 patients. Radiology. 2000. 216:704–111.
Article40. Burling D, Taylor SA, Halligan S, Gartner L, Paliwalla M, Peiris C, Singh L, Bassett P, Bartram C. Automated insufflation of carbon dioxide for MDCT colonography: distension and patient experience compared with manual insufflation. AJR Am J Roentgenol. 2006. 186:96–103.
Article41. Gryspeerdt SS, Herman MJ, Baekelandt MA, van Holsbeeck BG, Lefere PA. Supine/left decubitus scanning: a valuable alternative to supine/prone scanning in CT colonography. Eur Radiol. 2004. 14:768–777.
Article42. Laghi A, Iannaccone R, Mangiapane F, Piacentini F, Iori S, Passariello R. Experimental colonic phantom for the evaluation of the optimal scanning technique for CT colonography using a multidetector spiral CT equipment. Eur Radiol. 2003. 13:459–466.
Article43. Wessling J, Fischbach R, Meier N, Allkemper T, Klusmeier J, Ludwig K, Heindel W. CT colonography: Protocol optimization with multi-detector row CT-study in an anthropomorphic colon phantom. Radiology. 2003. 228:753–759.
Article44. Taylor SA, Halligan S, Bartram CI, Morgan PR, Talbot IC, Fry N, Saunders BP, Khosraviani K, Atkin W. Multi-detector row CT colonography: effect of collimation, pitch, and orientation on polyp detection in a human colectomy specimen. Radiology. 2003. 229:109–118.
Article45. Barish MA, Soto JA, Ferrucci JT. Consensus on current clinical practice of virtual colonoscopy. AJR. 2005. 184:786–792.
Article46. Kim SH, Lee JM, Eun HW. 2D versus 3D colonic evaluation using new virtual dissection software for CT colonography. Radiology. in press.47. Zalis ME, Barish MA, Choi JR, Dachman AH, Fenlon HM, Ferrucci JT, Glick SN, Laghi A, Macari M, McFarland EG, Morrin MM, Pickhardt PJ, Soto J, Yee J. Working Group on Virtual Colonoscopy. CT colonography reporting and data system: a consensus proposal. Radiology. 2005. 236:3–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Virtual CT Colonoscopy and Virtual CT Barium Enema using Multidetector-row CT
- Utility of CT colonography in detecting colon polyps as a colon cancer screen
- Efficacy of CT Colonography in the Detection of Colorectal Polypoid Lesions
- A Comparison of Patient Acceptance and Preferences Between CT Colonography and Conventional Colonoscopy in Colorectal Cancer Screening
- Diagnostic Performance of CT Colonography for the Detection of Colorectal Polyps
