J Korean Med Assoc.
2006 Nov;49(11):1027-1034. 10.5124/jkma.2006.49.11.1027.
Whole Body Positron Emission Tomography/Computed Tomography
- Affiliations
-
- 1Department of Nuclear Medicine, Sungkyunkwan University School of Medicine, Korea. jynm.choi@samsung.com, btnm.kim@samsung.com
- KMID: 2184726
- DOI: http://doi.org/10.5124/jkma.2006.49.11.1027
Abstract
- Whole body positron emission tomography (PET) using F-18 Fluorodeoxyglucose (FDG) has been used for characterizing focal lesions, initial staging, monitoring recurrence, and post-therapeutic follow-up in various malignant tumors. A recently developed integrated PET/computed tomography (CT) scanner is able to perform hardware-based image fusion of functional PET and anatomical CT images with ease and high registration accuracy. F-18 FDG PET/CT is more useful than conventional PET due to the shorter scan time and easy differential diagnosis between physiological and pathological uptake, allowing for accurate anatomical localization, improved diagnostic confidence and accuracy, and better radiation therapy planning. The application of F-18 FDG PET/CT in oncology practice is on its sharp rise in Korea due to the recent change of the reimbursement system to allow insurance coverage along with its wide range of clinical utilities. Whole body PET/CT deserves a particular attention as a useful diagnostic imaging modality in oncology practice.
MeSH Terms
Figure
-
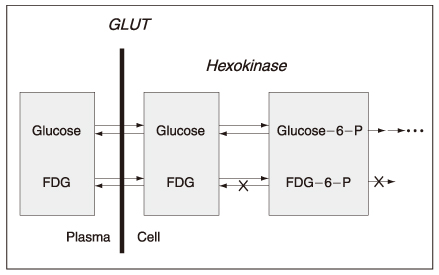
Figure 1 Cellular uptake mechanism of F-18 FDG as a PET tracer compared with that of glucose
Figure 2 Representative example of a commercialized integrated PET/CT scanner

Figure 3 A 60-year-old female patient with right lung cancer had an abnormal focal F-18 FDG uptake in the right lower neck area mimicking N3 lymph node metastasis. However, fused PET/CT images revealed that it was a focal lesion in the right thyroid gland, which was proved to be a papillary thyroid cancer by fine needle aspiration cytology and biopsy
Reference
-
2. Townsend DW, Carney JP, Yap JT, Hall NC. PET/CT today and tomorrow. J Nucl Med. 2004. 45:4S–14S.3. Tian M, Zhang H, Nakasone Y, Mogi K, Endo K. Expression of Glut-1 and Glut-3 in untreated oral squamous cell carcinoma compared with FDG accumulation in a PET study. Eur J Nucl Med Mol I. 2004. 31:5–12.
Article4. Tohma T, Okazumi S, Makino H, Cho A, Mochiduki R, Ochiai T, et al. Relationship between glucose transporter, hexokinase and FDG-PET in esophageal cancer. Hepato-Gastroentero. 2005. 52:486–490.5. Nakamoto Y, Osman M, Cohade C, Marshall LT, Links JM, Wahl RL, et al. PET/CT: comparison of quantitative tracer uptake between germanium and CT transmission attenuation-corrected images. J Nucl Med. 2002. 43:1137–1143.6. Beyer T, Antoch G, Muller S, Egelhof T, Freudenberg LS, Bockisch A, et al. Acquisition protocol considerations for combined PET/CT imaging. J Nucl Med. 2004. 45:25S–35S.7. Vogel WV, Oyen WJ, Barentsz JO, Kaanders JH, Corstens FH. PET/CT: panacea, redundancy, or something in between? J Nucl Med. 2004. 45:15S–24S.8. Gambhir SS, Czernin J, Schwimmer J, Silverman DH, Coleman RE, Phelps ME. A tabulated summary of the FDG PET literature. J Nucl Med. 2001. 42:1S–93S.10. Sasaki R, Komaki R, Macapinlac H, Erasmus J, Allen P, Cox JD, et al. [18F]fluorodeoxyglucose uptake by positron emission tomography predicts outcome of non-small-cell lung cancer. J Clin Oncol. 2005. 23:1136–1143.
Article11. Choi JY, Jang HJ, Shim YM, Kim K, Lee KS, Kim BT, et al. 18F-FDG PET in patients with esophageal squamous cell carcinoma undergoing curative surgery: prognostic implications. J Nucl Med. 2004. 45:1843–1850.13. Bar-Shalom R, Yefremov N, Guralnik L, Gaitini D, Frenkel A, Israel O, et al. Clinical performance of PET/CT in evaluation of cancer: additional value for diagnostic imaging and patient management. J Nucl Med. 2003. 44:1200–1209.14. Schoder H, Yeung HW, Gonen M, Kraus D, Larson SM. Head and neck cancer: clinical usefulness and accuracy of PET/CT image fusion. Radiology. 2004. 231:65–72.
Article15. Lardinois D, Weder W, Hany TF, Kamel EM, Korom S, Steinert HC, et al. Staging of non-small-cell lung cancer with integrated positron emission tomography and computed tomography. New Engl J Med. 2003. 348:2500–2507.
Article16. Menda Y, Graham MM. Update on 18F-fluorodeoxy-glucose/positron emission tomography and positron emission tomography/computed tomography imaging of squamous head and neck cancers. Semin Nucl Med. 2005. 35:214–219.
Article17. Yuan S, Yu Y, Chao KS, Fu Z, Yin Y, Yu J, et al. Additional value of PET/CT over PET in assessment of locoregional lymph nodes in thoracic esophageal squamous cell cancer. J Nucl Med. 2006. 47:1255–1259.18. Choi JY, Lee KS, Kwon OJ, Shim YM, Baek CH, Kim BT, et al. Improved detection of second primary cancer using integrated [18F] fluorodeoxyglucose positron emission tomography and computed tomography for initial tumor staging. J Clin Oncol. 2005. 23:7654–7659.
Article19. van Der Wel A, Nijsten S, Hochstenbag M, Lamers R, Boersma L, De Ruysscher D, et al. Increased therapeutic ratio by 18FDG-PET CT planning in patients with clinical CT stage N2-N3M0 non-small-cell lung cancer: a modeling study. Int J Radiat Oncol. 2005. 61:649–655.
Article20. Brianzoni E, Rossi G, Ancidei S, Berbellini A, Capoccetti F, Algranati C, et al. Radiotherapy planning: PET/CT scanner performances in the definition of gross tumour volume and clinical target volume. Eur J Nucl Med Mol Imaging. 2005. 32:1392–1399.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- 18F-2-Deoxy-2-Fluoro-D-Glucose Positron Emission Tomography: Computed Tomography for Preoperative Staging in Gastric Cancer Patients
- Nuclear Medicine Imaging in Rheumatic Diseases
- Oral cancer diagnosed using PET/CT: A case report
- Applicationof Positron Emission Tomography in Gastrointestimal Carcinomas
- Clinical Application of Positron Emission Tomography
