Comparison of the Impact of the Anesthesia Induction Using Thiopental and Propofol on Cardiac Function for Non-Cardiac Surgery
- Affiliations
-
- 1Department of Cardiovascular Medicine, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea.
- 2Department of Anesthesiology, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea. taeyop@gmail.com
- 3Department of Cardiovascular Surgery, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea.
- 4Department of Obstetrics and Gynecology, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea.
- 5Department of General Surgery, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea.
- KMID: 2177460
- DOI: http://doi.org/10.4250/jcu.2014.22.2.58
Abstract
- BACKGROUND
Thiopental and propofol have been widely used for general anesthesia induction, but their impacts on cardiac function have not been well described. A recent study speculated that anesthesia induction using propofol 2 mg/kg transiently reduced left ventricular (LV) contraction by analyzing tissue Doppler-derived imaging (TDI) during induction phase. The purpose of this study was to analyze and to compare the impacts of propofol- and thiopental-induction on LV function.
METHODS
Twenty-four female patients with normal LV function undergoing non-cardiac surgery were randomly administered intravenous bolus thiopental (5 mg/kg, Thiopental-group, n = 12) or propofol (2 mg/kg, Propofol-group, n = 12) for anesthesia-induction. TDI of septal mitral annular velocity during systole (S'), early diastole (e') and atrial contraction (a') were determined by transthoracic echocardiography before and 1, 3, and 5 minutes after thiopental/propofol administration (T0, T1, T2, and T3, respectively).
RESULTS
The bispectral index and systolic blood pressure declined significantly during anesthesia induction in both groups, however, more depressed in Thiopental-group compared with those in Propofol-group at T2 and T3 (all, p < 0.05). Among TDI two parameters demonstrated a significant inter-group difference: the S' in propofol was lower than that in Thiopental-group at T3 (p = 0.002), and a' velocities were persistently lower in Propofol-group, compared with same time values in Thiopental-group (T1, T2, and T3: p = 0.025, 0.007, and 0.009, respectively).
CONCLUSION
Anesthesia induction using propofol revealed a more persistent and profound decline of LV and atrial contraction than that using thiopental. Further studies are needed to understand the clinical implication.
Keyword
MeSH Terms
Figure
-
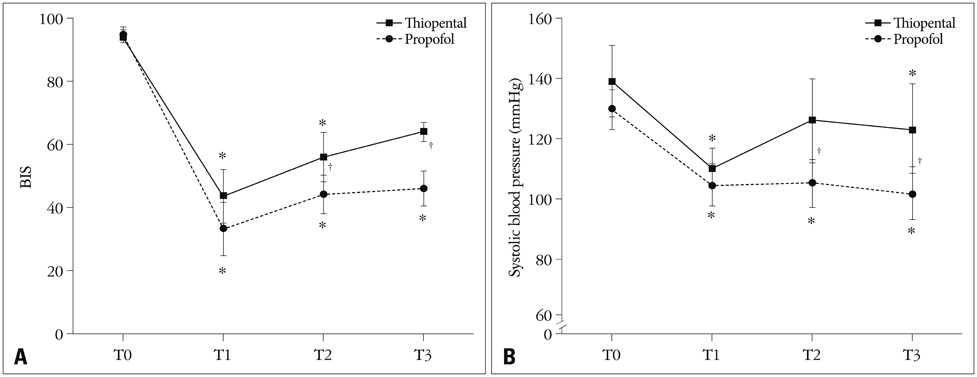
Fig. 1 Comparison of serial hemodynamic changes between Thiopental and Propofol group. Serial bispectral index (BIS) (A), and systolic blood pressure (B) in the thiopental and propofol group, before and 1, 3, and 5 minutes after injection of anesthesia (T0, T1, T2, and T3, respectively). Thiopental: patients administered bolus thiopental 5.0 mg/kg, Propofol: patients administered bolus propofol 2.0 mg/kg. Values were median (interquartile). *p < 0.05 vs. T0 within the group by Friedman's test with multiple comparisons, †p < 0.05, between the group by the Wilcoxon-Mann-Whitney test. A significant group difference is noted 3 to 5 minutes after anesthesia injection.
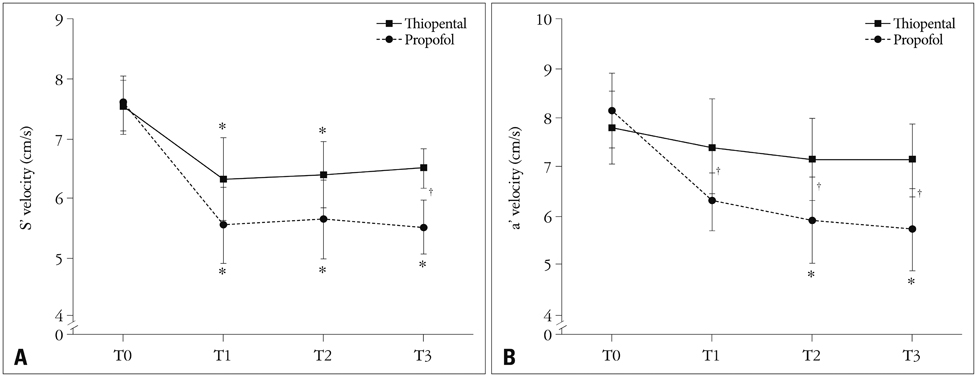
Fig. 2 Comparison of tissue Doppler-derived indices of septal mitral annular velocity during systole (S') and late diastole atrial contraction (a'). Serial S' velocities (A), and a' velocities (B) in Thiopental and Propofol group, before and 1, 3, and 5 minutes after injection of anesthesia (T0, T1, T2, and T3, respectively). Thiopental: patients administered bolus thiopental 5.0 mg/kg, Propofol: patients administered bolus propofol 2.0 mg/kg. Values were median (interquartile). *p < 0.05, vs. T0 within the group by Friedman's test with multiple comparisons, †p < 0.05, between the group. Persistent decline of S' (compared with T0) is noted at T3 in the propofol group, which is recovered in the thiopental. At T3, the S' is lower in propofol than in thiopental (p = 0.002). Declining of a' velocities from T0 is significant throughout the study period in the propofol group; however, those changes are not observed in the thiopental group (p < 0.05).
Cited by 2 articles
-
Isoflurane's Effect on Intraoperative Systolic Left Ventricular Performance in Cardiac Valve Surgery Patients
Ju Deok Kim, Ilsoon Son, Won-kyoung Kwon, Tae-Yun Sung, Hanafi Sidik, Karam Kim, Hyun Kang, Jiyon Bang, Gwi Eun Yeo, Dong Kyu Lee, Tae-Yop Kim
J Korean Med Sci. 2018;33(4):. doi: 10.3346/jkms.2018.33.e28.Pharmacodynamic Analysis of the Influence of Propofol on Left Ventricular Long-Axis Systolic Performance in Cardiac Surgical Patients
Ji-Yeon Bang, Sooyoung Kim, Byung-Moon Choi, Tae-Yop Kim
J Korean Med Sci. 2019;34(16):. doi: 10.3346/jkms.2019.34.e132.
Reference
-
1. Singh A, Antognini JF. Perioperative hypotension and myocardial ischemia: diagnostic and therapeutic approaches. Ann Card Anaesth. 2011; 14:127–132.
Article2. American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. American Society of Echocardiography. American Society of Nuclear Cardiology. Heart Rhythm Society. Society for Cardiovascular Angiography and Interventions. Society for Vascular Medicine. Society of Cardiovascular Anesthesiologists. Society for Vascular Surgery. Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof EL, Fleischmann KE, Freeman WK, Froehlich JB, Kasper EK, Kersten JR, Riegel B, Robb JF. 2009 ACCF/AHA focused update on perioperative beta blockade incorporated into the ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery. J Am Coll Cardiol. 2009; 54:e13–e118.
Article3. Task Force for Preoperative Cardiac Risk Assessment and Perioperative Cardiac Management in Non-cardiac Surgery. European Society of Cardiology (ESC). Poldermans D, Bax JJ, Boersma E, De Hert S, Eeckhout E, Fowkes G, Gorenek B, Hennerici MG, Iung B, Kelm M, Kjeldsen KP, Kristensen SD, Lopez-Sendon J, Pelosi P, Philippe F, Pierard L, Ponikowski P, Schmid JP, Sellevold OF, Sicari R, Van den Berghe G, Vermassen F. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery. Eur Heart J. 2009; 30:2769–2812.
Article4. Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, Sugarbaker DJ, Donaldson MC, Poss R, Ho KK, Ludwig LE, Pedan A, Goldman L. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999; 100:1043–1049.
Article5. Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof EL, Fleischmann KE, Freeman WK, Froehlich JB, Kasper EK, Kersten JR, Riegel B, Robb JF, Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Buller CE, Creager MA, Ettinger SM, Faxon DP, Fuster V, Halperin JL, Hiratzka LF, Hunt SA, Lytle BW, Nishimura R, Ornato JP, Page RL, Riegel B, Tarkington LG, Yancy CW. ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery) Developed in Collaboration With the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. J Am Coll Cardiol. 2007; 50:1707–1732.6. Reich DL, Hossain S, Krol M, Baez B, Patel P, Bernstein A, Bodian CA. Predictors of hypotension after induction of general anesthesia. Anesth Analg. 2005; 101:622–628. table of contents.
Article7. Bovill JG. Intravenous anesthesia for the patient with left ventricular dysfunction. Semin Cardiothorac Vasc Anesth. 2006; 10:43–48.
Article8. Isaaz K. Tissue Doppler imaging for the assessment of left ventricular systolic and diastolic functions. Curr Opin Cardiol. 2002; 17:431–442.
Article9. Yang HS, Song BG, Kim JY, Kim SN, Kim TY. Impact of propofol anesthesia induction on cardiac function in low-risk patients as measured by intraoperative Doppler tissue imaging. J Am Soc Echocardiogr. 2013; 26:727–735.
Article10. Larsen JR, Torp P, Norrild K, Sloth E. Propofol reduces tissue-Doppler markers of left ventricle function: a transthoracic echocardiographic study. Br J Anaesth. 2007; 98:183–188.
Article11. Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, Waggoner AD, Flachskampf FA, Pellikka PA, Evangelista A. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr. 2009; 22:107–133.
Article12. Gauss A, Heinrich H, Wilder-Smith OH. Echocardiographic assessment of the haemodynamic effects of propofol: a comparison with etomidate and thiopentone. Anaesthesia. 1991; 46:99–105.
Article13. Mulier JP, Wouters PF, Van Aken H, Vermaut G, Vandermeersch E. Cardiodynamic effects of propofol in comparison with thiopental: assessment with a transesophageal echocardiographic approach. Anesth Analg. 1991; 72:28–35.14. Wodey E, Chonow L, Beneux X, Azzis O, Bansard JY, Ecoffey C. Haemodynamic effects of propofol vs thiopental in infants: an echocardiographic study. Br J Anaesth. 1999; 82:516–520.
Article15. Sørensen MK, Dolven TL, Rasmussen LS. Onset time and haemodynamic response after thiopental vs. propofol in the elderly: a randomized trial. Acta Anaesthesiol Scand. 2011; 55:429–434.
Article16. Aronson WL, McAuliffe MS, Miller K. Variability in the American Society of Anesthesiologists Physical Status Classification Scale. AANA J. 2003; 71:265–274.17. Tramèr MR, Moore RA, McQuay HJ. Propofol and bradycardia: causation, frequency and severity. Br J Anaesth. 1997; 78:642–651.
Article18. Park WK, Lynch C 3rd. Propofol and thiopental depression of myocardial contractility. A comparative study of mechanical and electrophysiologic effects in isolated guinea pig ventricular muscle. Anesth Analg. 1992; 74:395–405.
Article19. Chen WH, Lee CY, Hung KC, Yeh FC, Tseng CC, Shiau JM. The direct cardiac effect of propofol on intact isolated rabbit heart. Acta Anaesthesiol Taiwan. 2006; 44:19–23.20. Russo H, Bressolle F. Pharmacodynamics and pharmacokinetics of thiopental. Clin Pharmacokinet. 1998; 35:95–134.
Article21. Komai H, Rusy BF. Differences in the myocardial depressant action of thiopental and halothane. Anesth Analg. 1984; 63:313–318.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Thiopental Sodium and Propofol as Anesthetic Induction Agents for Hypnotic Time
- Comparision of Propofol and Thiopental for Electroconvulsive Therapy: Effects on Hemodynamic Changes and Intraocular Pressure
- A comparison of hemodynamics in elderly patients that were administered thiopental sodium or propofol to induce general anesthesia
- A Comparison between Propofol and Thiopental for Induction of Anesthesia for Elective Caesarean Section
- Comparison of Propofol and Thiopental Anesthesia for Ambulatory Surgery
