An Endobronchial Metastasis from Breast Cancer Seven Years after Modified Radical Mastectomy: A Case Report
- Affiliations
-
- 1Department of Internal Medicine, The Catholic University of Korea, College of Medicine, Seoul, Korea. mdlee@catholic.ac.kr
- 2Department of Pathology, The Catholic University of Korea, College of Medicine, Seoul, Korea.
- 3Department of Diagnostic Radiology, The Catholic University of Korea, College of Medicine, Seoul, Korea.
- 4Department of Thoracic and Cardiovacular Surgery, The Catholic University of Korea, College of Medicine, Seoul, Korea.
- 5Department of Surgery, The Catholic University of Korea, College of Medicine, Seoul, Korea.
- KMID: 2175212
- DOI: http://doi.org/10.4048/jbc.2009.12.2.113
Abstract
- A 39-year-old woman was admitted to our hospital because of her chronic cough. She had undergone modified radical mastectomy for breast cancer 7 year before admission. A chest radiograph showed collapse of the left upper lobe (LUL) and computed tomography of the chest revealed a mass in the proximal portion of the LUL bronchus and distal atelectasis. Bronchoscopy showed obstruction of the LUL bronchus. The microscopic examination showed findings consistent with breast cancer with the same immunohistochemical features for the hormone receptors, as compared to those features of the previously resected tumor. Positron emission tomography showed increased fluorodeoxyglucose uptake only in the LUL. Left upper lobectomy was performed and she is now undergoing systemic chemotherapy. We report here on this rare case to emphasize that when a patient with a history of breast cancer complains of respiratory symptoms, and even though the patient was treated curatively a long time ago, we should suspect the possibility of endobronchial metastasis.
MeSH Terms
Figure
-
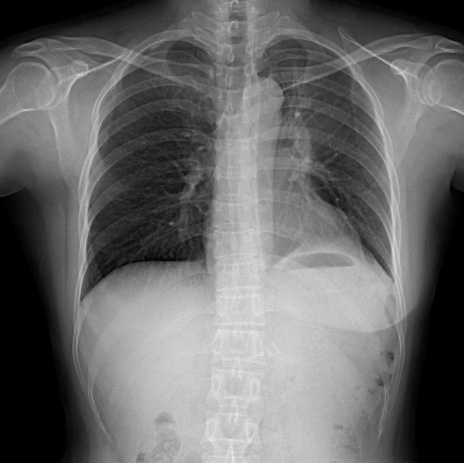
Figure 1 A posteroanterior chest radiograph shows a poorly defined increased opacity in left suprahilar area and superior displacement of the left hilum, suggesting collapse of left upper lobe.

Figure 2 A contrast medium-enhanced computed tomography scan demonstrates a space occupying lesion (arrows) in left upper lobar bronchus and resultant atelectasis of left upper lobe.
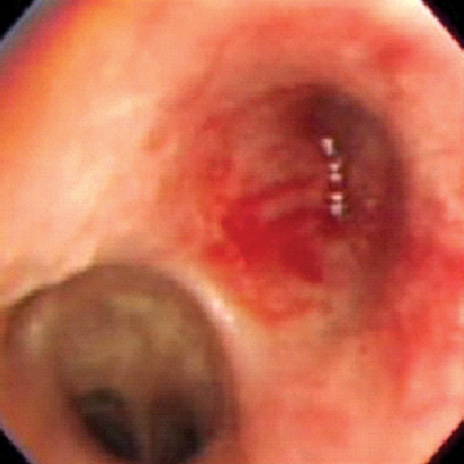
Figure 3 Flexible bronchoscopy shows obstruction of left upper lobar bronchus with hyperemic mucosal change.
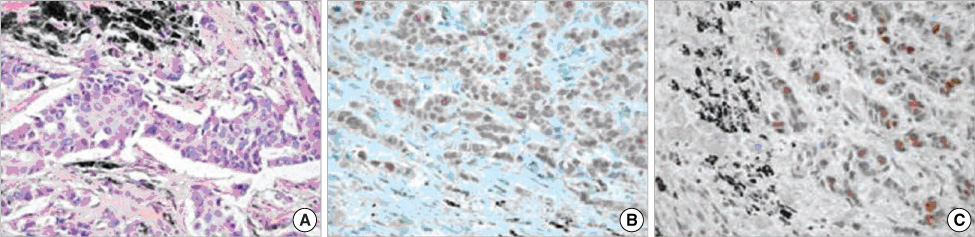
Figure 4 Microscopic examinations of bronchoscopic biopsy specimen shows pleomorphic, poorly differentiated carcinoma (A, H&E stain, ×400). Immunohistochemical stain demonstrates positive reactivity to both estrogen (B, ×400) and progesterone receptors (C, ×400).
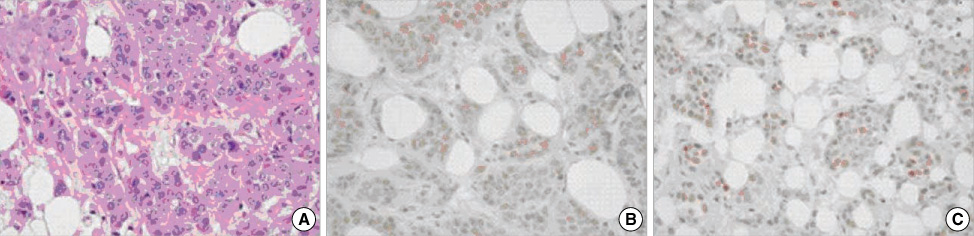
Figure 5 Microscopic examinations of mastectomy specimen shows poorly differentiated adenocarcinoma (A, H&E stain, ×400). Immunohistochemical stain demonstrates positive reactivity to both estrogen (B, ×400) and progesterone receptors (C, ×400).
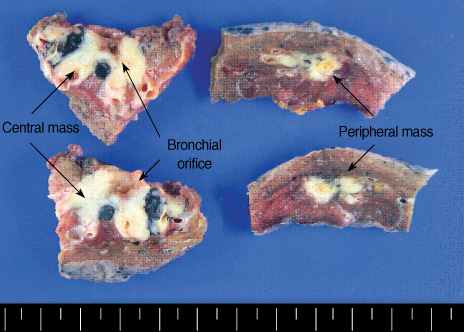
Figure 6 Left upper lobectomy specimen shows two ivory colored masses. Left upper lobe is obstructed by a larger mass, measured 3.0×2.0 cm in size and another one, 2.0×1.0 cm in size is located in the peripheral lung parenchyme.
Reference
-
1. Rosenblatt MB, Lisa JR, Trinidad S. Pitfalls in the clinical histologic diagnosis of bronchogenic carcinoma. Dis Chest. 1966. 49:396–404.
Article2. Braman SS, Whitcomb ME. Endobronchial metastasis. Arch Intern Med. 1975. 135:543–547.
Article3. Baumgartner WA, Mark JB. Metastatic malignancies from distant sites to the tracheobronchial tree. J Thorac Caridovasc Surg. 1980. 79:499–503.
Article4. Kim DH, Park MS, Chung JH, Cheong JH, Kim SK, Chang J, et al. Endobronchial metastasis of extrapulmonary malignancies. Tuberc Respir Dis. 2002. 53:285–293.
Article5. Park KH, Kim SI, Ko SS, Park BW, Lee KS. The pattern of systemic failure and factors influencing on the outcome after distant metastasis in breast cancer. J Korean Breast Cancer Soc. 2003. 6:109–116.
Article6. Hagemeister FB, Buzbar AV, Luna MA. Cause of death in breast cancer. Cancer. 1980. 46:162–167.7. DeBeer RA, Garcia RI, Alexander SC. Endobronchial metastasis from cancer of the breast. Chest. 1978. 73:94–96.
Article8. Kiryu T, Hoshi H, Matsui E. Endotracheal/endobronchial metastases. Chest. 2001. 119:768–775.
Article9. Berg HK, Petrelli NJ, Herrera L, Lopez C, Mittelman A. Endobronchial metastasis from colorectal carcinoma. Dis Colon Rectum. 1984. 27:745–748.
Article10. Salud A, Porcel JM, Rovirosa A, Bellmunt J. Endobronchial metastatic disease. J Surg Oncol. 1996. 62:249–252.
Article11. Beasley MB. Immunohistochemistry of pulmonary and pleural neoplasia. Arch Pathol Lab Med. 2008. 132:1062–1072.
Article12. Horing HM, van Laar RK, Kerst JM, Hegason HH, Weseling J, van der Hoeven JJ, et al. Gene expression profiling to identify the histogenetic origin of metastatic adenocarcinomas of unknown primary. J Clin Oncol. 2008. 26:4435–4441.
Article13. Katsimbri PP, Bamias AT, Froudarakis ME, Peponis IA. Endobronchial metastases secondary to solid tumors. Lung Cancer. 2000. 28:163–170.
