Two Cases of Gastrocolocutaneous Fistula with a Long Asymptomatic Period after Percutaneous Endoscopic Gastrostomy
- Affiliations
-
- 1Department of Internal Medicine, Hallym University College of Medicine, Chuncheon, Korea. kimyeonsoo@hallym.or.kr
- KMID: 2174385
- DOI: http://doi.org/10.5217/ir.2014.12.3.251
Abstract
- Gastrocolocutaneous fistula is a rare complication of the percutaneous endoscopic gastrostomy (PEG) procedure. Typical symptoms usually occur in the first few months. We recently encountered 2 patients with 8- and 33-month asymptomatic periods. A 74-year-old man presented with watery diarrhea for 1 month. He had undergone PEG 9 months earlier. During workup, an upper endoscopy and abdominal CT scan revealed the migration of the feeding tube into the transverse colon. He was discharged with a nasogastric tube after treatment. A 77-year-old man presented with sudden loosening of his PEG tube with a duration over 3 days. He had undergone PEG procedure three times until that time. During workup, a gastrocolocutaneous fistula was diagnosed. However, when previous studies were reviewed, an abdominal CT scan, which was done 6 months ago before the third PEG, showed the fistula already existed at that time, suggesting that it was created about 33 months earlier when he underwent the second PEG procedure. The patient died of pneumonia aggravation despite conservative treatment. Both a high index of suspicion and the careful inspection of the upper endoscopy are very important for early diagnosis regardless of symptoms.
MeSH Terms
Figure
-
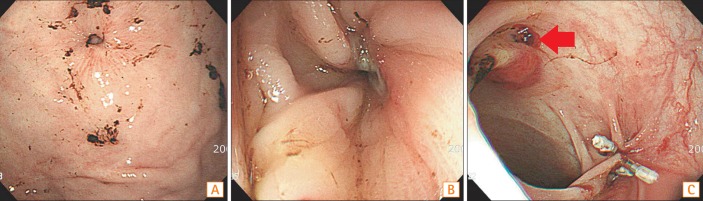
Fig. 1 Gastric and colonic view of fistula. (A) Upper endoscopy revealed a gastrocolic fistula and no visible bumper of the internal percutaneous endoscopic gastrostomy (PEG) tube. (B) Colonoscopy revealed a gastrocolic fistula in the transverse colon. (C) Three metal clips were successfully placed at the gastrocolic fistula opening during colonoscopy. The red arrow indicates the colocutaneous fistula opening, which remained under observation for spontaneous closure.

Fig. 2 Abdominal CT findings. (A) The bumper of the feeding tube that migrated into the colonic lumen (axial view). (B) The white arrow indicates the fistula's tract between A B the stomach and colon (sagittal view).

Fig. 3 Endoscopic sealing of the fistula. A radiologic study with gastrografin administered through a nasogastric tube was performed 1 week after the colonoscopic metal clipping. There was no leakage of dye from the stomach. The white arrow indicates the previous metal clips located at the colonic opening of the gastrocolic fistula.

Fig. 4 Upper endoscopic findings. (A) An upper endoscopy which was done 6 months ago. The gastrocolocutaneous fistula was misdiagnosed as buried-bumper syndrome 6 months previously. (B) An upper endoscopy which was done at this time. The bumper of the feeding tube was deeply buried within the gastric wall and had formed a hole at the time of the patient's admission to our hospital. (C) The bumper with fecal material observed through the gastrocolic fistula. A large space was observed when the scope was advanced into the hole, and brownish material was attached to the bumper. (D) The colonic lumen observed through the gastrocolic fistula. The colonic lumen was identified by a bluish liver shadow and colonic haustra, 3 weeks later.

Fig. 5 Schematic diagrams of the 3 stages based on the position of the bumper in Case 2. (A) The gastrocolocutaneous fistula was created during the percutaneous endoscopic gastrostomy (PEG) placement, and the transverse colon was pressed tightly between the stomach and the abdominal wall (the first stage). (B) During the intervening period, the transmural migration of the feeding tube showed endoscopic findings similar to those of buried-bumper syndrome (the second stage). (C) The bumper migrated into the intracolonic space through the gastrocolic fistula (the third stage).
Cited by 1 articles
-
Gastrocolocutaneous Fistula: An Unusual Case of Gastrostomy Tube Malfunction with Diarrhea
Junghwan Lee, Jinyoung Kim, Ha il Kim, Chung Ryul Oh, Sungim Choi, Soomin Noh, Hee Kyong Na, Hwoon-Yong Jung
Clin Endosc. 2018;51(2):196-200. doi: 10.5946/ce.2017.062.
Reference
-
1. Berger SA, Zarling EJ. Colocutaneous fistula following migration of PEG tube. Gastrointest Endosc. 1991; 37:86–88. PMID: 1900799.
Article2. Blomberg J, Lagergren J, Martin L, Mattsson F, Lagergren P. Complications after percutaneous endoscopic gastrostomy in a prospective study. Scand J Gastroenterol. 2012; 47:737–742. PMID: 22471958.
Article3. Croaker GD, Najmaldin AS. Laparoscopically assisted percutaneous endoscopic gastrostomy. Pediatr Surg Int. 1997; 12:130–131.
Article4. Pitsinis V, Roberts P. Gastrocolic fistula as a complication of percutaneous endoscopic gastrostomy. Eur J Clin Nutr. 2003; 57:876–878. PMID: 12821887.
Article5. Huang SY, Levine MS, Raper SE. Gastrocolic fistula with migration of feeding tube into transverse colon as a complication of percutaneous endoscopic gastrostomy. AJR Am J Roentgenol. 2005; 184:S65–S66. PMID: 15728025.
Article6. Lenzen H, Weismuller T, Bredt M, Bahr M. Education and imaging. Gastrointestinal: PEG feeding tube migration into the colon; a late manifestation. J Gastroenterol Hepatol. 2012; 27:1254. PMID: 22712710.
Article7. Marcy PY, Magne N, Lacroix J, Bailet C. Late presentation of a gastrocolic fistula after percutaneous fluoroscopic gastrostomy. JBR-BTR. 2004; 87:17–20. PMID: 15055328.8. Naehrlich L, Carbon R, Lang T, Behrens R. Two rare complications of percutaneous endoscopic gastrostomy: obstruction of the pylorus and gastrocolic fistula occurring in one patient. Klin Padiatr. 2001; 213:329–331. PMID: 11713711.
Article9. Minocha A, Rupp TH, Jaggers TL, Rahal PS. Silent colo-gastrocutaneous fistula as a complication of percutaneous endoscopic gastrostomy. Am J Gastroenterol. 1994; 89:2243–2244. PMID: 7977251.10. Payne KM, King TM, Eisenach JB. The technique of percutaneous endoscopic gastrostomy. A safe and cost-effective alternative to operative gastrostomy. J Crit Illn. 1991; 6:611–619. PMID: 10147918.11. McClave SA, Chang WK. Complications of enteral access. Gastrointest Endosc. 2003; 58:739–751. PMID: 14595312.
Article12. Foutch PG, Talbert GA, Waring JP, Sanowski RA. Percutaneous endoscopic gastrostomy in patients with prior abdominal surgery: virtues of the safe tract. Am J Gastroenterol. 1988; 83:147–150. PMID: 3124605.13. Holder TM, Leape LL, Ashcraft KW. Gastrostomy: its use and dangers in pediatric patients. N Engl J Med. 1972; 286:1345–1347. PMID: 4554838.
Article14. Joo YJ, Koo JH, Song SH. Gastrocolic fistula as a cause of persistent diarrhea in a patient with a gastrostomy tube. Arch Phys Med Rehabil. 2010; 91:1790–1792. PMID: 21044727.
Article15. Okutani D, Kotani K, Makihara S. A case of gastrocolocutaneous fistula as a complication of percutaneous endoscopic gastrostomy. Acta Med Okayama. 2008; 62:135–138. PMID: 18464890.16. Hwang JH, Kim HW, Kang DH, et al. A case of endoscopic treatment for gastrocolocutaneous fistula as a complication of percutaneous endoscopic gastrostomy. Clin Endosc. 2012; 45:95–98. PMID: 22741139.
Article17. Lynch CR, Fang JC. Prevention and management of complications of percutaneous endoscopic gastrostomy (PEG) tubes. Pract Gastroenterol. 2004; 28:66–77.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Gastrocolocutaneous Fistula Caused by Percutaneous Endoscopic Gastrostomy
- Two Cases of Uncommon Complication during Percutaneous Endoscopic Gastrostomy Tube Replacement and Treatment
- A Case of Endoscopic Treatment for Gastrocolocutaneous Fistula as a Complication of Percutaneous Endoscopic Gastrostomy
- Gastrocolocutaneous Fistula: An Unusual Case of Gastrostomy Tube Malfunction with Diarrhea
- Long Term Efficacy of Percutaneous Endoscopic Gastrostomy
