Treatment of a Ruptured Vertebrobasilar Fusiform Aneurysm Using Pipeline Embolization Device
- Affiliations
-
- 1Department of Neurosurgery, Rush University Medical Center, Chicago, IL, USA. roham_moftakhar@rush.edu
- KMID: 2172028
- DOI: http://doi.org/10.7461/jcen.2013.15.1.30
Abstract
- Treatment options of ruptured vertebrobasilar fusiform aneurysms (VFA) are limited and often carry significant mortality and morbidity. We report the use of Pipeline Embolization Device (PED) to successfully treat a patient with a ruptured vertebrobasilar fusiform aneurysm (VFA) who presented with subarachnoid hemorrhage (SAH). A 73 year-old man with a history of cardiac stent placement seven days earlier presented with Hunt-Hess II SAH. He was taking aspirin and clopidogrel. Computed tomography angiogram revealed a large vertebrobasilar fusiform aneurysm. Microsurgical treatment options are technically challenging and carry high risk. He underwent endovascular treatment of the ruptured VFA using overlapping PEDs. Five PEDs were placed in a telescoping fashion to reconstruct the affected portions of the left vertebral and basilar arteries. An additional 2-mm blister aneurysm in the right vertebral artery was also discovered during the conventional cerebral angiography and was treated with one additional PED. The patient remained neurologically intact after the procedure. He was continued on aspirin and clopidogrel. Follow-up magnetic resonance imaging at three months demonstrated patency of the stents without any evidence of ischemic change. Follow-up conventional cerebral angiogram at six months demonstrated thrombosis of the VFA and reconstruction of the vertebrobasilar system. The patient remained clinically well. An endovascular approach using PEDs can be a safe and effective treatment option for ruptured VFA in selected cases.
Keyword
MeSH Terms
Figure
-
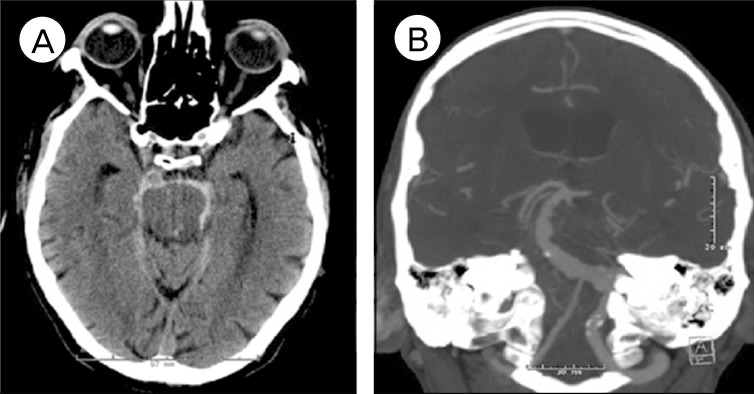
Fig. 1 Computed tomography (CT) of the brain without contrast (left) showing subarachnoid hemorrhage in the prepontine, ambient and crural cisterns; CT angiogram of the brain (right) showing a vertebrobasilar fusiform aneurysm, also known as vertebrobasilar dolichoectasia involving the left vertebral and basilar arteries. The right vertebral artery is irregular and non-dominant.
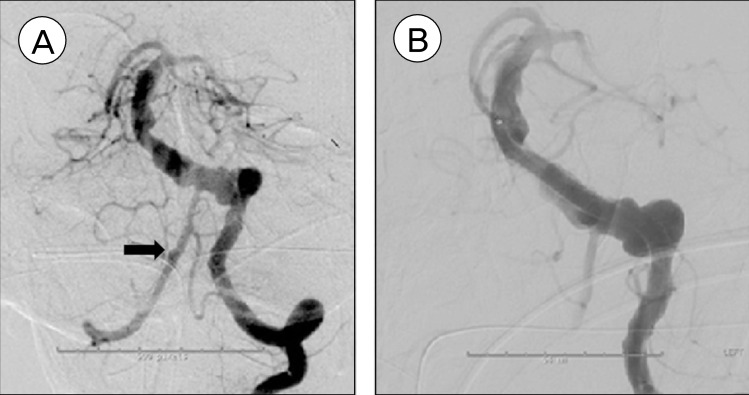
Fig. 2 Pretreatment conventional cerebral angiogram (left) demonstrating fusiform dilation of the left vertebral and basilar arteries, along with a 2 mm blister aneurysm (arrow) in the right vertebral artery proximal to posterior inferior cerebellar artery takeoff; post-treatment angiogram (right) demonstrating reconstruction of affected vessel lumen and stasis of blood flow in the irregular portion of the vessels outside of Pipeline Embolization Device construct.
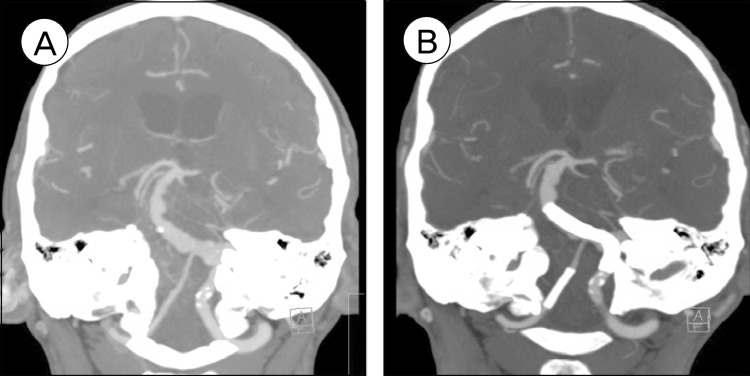
Fig. 3 Comparison of pretreatment CT angiogram (left) and CT angiogram on post operative day five (right), demonstrating patent vertebrobasilar system and reconstruction of the fusiform vertebrobasilar artery after treatment.
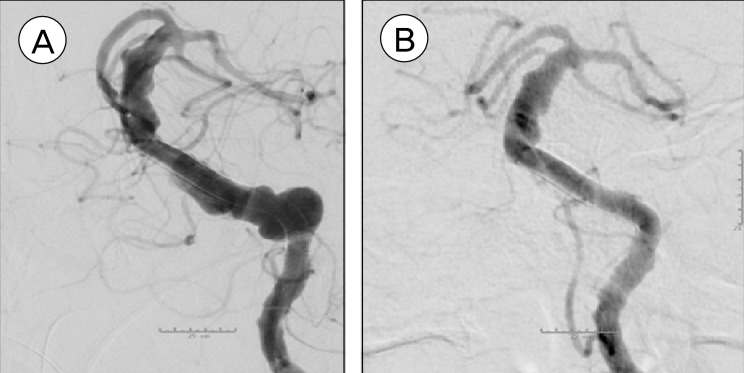
Fig. 4 Cerebral angiogram immediately after Pipeline embolization device placement (left); Follow-up cerebral angiogram at six-month after procedure (right) showing remodeling of left vertebral and basilar arteries and thrombosis of the vertebrobasilar fusiform aneurysm.
Cited by 1 articles
-
Ventriculoperitoneal Shunt in a Patient with Ruptured Blister Aneurysm Treated with Pipeline Embolization Device
Lee A. Tan, Carter S. Gerard, Kiffon M. Keigher, Roham Moftakhar, Demetrius K. Lopes
J Cerebrovasc Endovasc Neurosurg. 2015;17(1):54-58. doi: 10.7461/jcen.2015.17.1.54.
Reference
-
1. Fiorella D, Kelly ME, Albuquerque FC, Nelson PK. Curative reconstruction of a giant midbasilar trunk aneurysm with the pipeline embolization device. Neurosurgery. 2009; 2. 64(2):212–217. discussion 217. PMID: 19057425.
Article2. Kallmes DF, Ding YH, Dai D, Kadirvel R, Lewis DA, Cloft HJ. A second-generation, endoluminal, flow-disrupting device for treatment of saccular aneurysms. AJNR Am J Neuroradiol. 2009; 6. 30(6):1153–1158. PMID: 19369609.
Article3. Kallmes DF, Ding YH, Dai D, Kadirvel R, Lewis DA, Cloft HJ. A new endoluminal, flow-disrupting device for treatment of saccular aneurysms. Stroke. 2007; 8. 38(8):2346–2352. PMID: 17615366.
Article4. Mizutani T, Aruga T, Kirino T, Miki Y, Saito I, Tsuchida T. Recurrent subarachnoid hemorrhage from untreated ruptured vertebrobasilar dissecting aneurysms. Neurosurgery. 1995; 5. 36(5):905–911. discussion 912-3. PMID: 7791980.
Article5. Nelson PK, Lylyk P, Szikora I, Wetzel SG, Wanke I, Fiorella D. The pipeline embolization device for the in tracranial treatment of aneurysms trial. AJNR Am J Neuroradiol. 2011; 1. 32(1):34–40. PMID: 21148256.6. Passero SG, Calchetti B, Bartalini S. Intracranial bleeding in patients with vertebrobasilar dolichoectasia. Stroke. 2005; 7. 36(7):1421–1425. PMID: 15976311.
Article7. Siddiqui AH, Abla AA, Kan P, Dumont TM, Jahshan S, Britz GW, et al. Panacea or problem: flow diverters in the treatment of symptomatic large or giant fusiform vertebrobasilar aneurysms. J Neurosurg. 2012; 6. 116(6):1258–1266. PMID: 22404673.
Article8. Smoker WR, Corbett JJ, Gentry LR, Keyes WD, Price MJ, McKusker S. High-resolution computed tomography of the basilar artery: 2. Vertebrobasilar dolichoectasia: clinical-pathologic correlation and review. AJNR Am J Neuroradiol. 1986; Jan-Feb. 7(1):61–72. PMID: 3082145.9. Szikora I, Berentei Z, Kulcsar Z, Marosfoi M, Vajda ZS, Lee W, et al. Treatment of intracranial aneurysms by functional reconstruction of the parent artery: the Budapest experience with the pipeline embolization device. AJNR Am J Neuroradiol. 2010; 6. 31(6):1139–1147. PMID: 20150304.
Article10. Titlic M, Tonkic A, Jukic I, Kolic K, Dolic K. Clinical manifestations of vertebrobasilar dolichoectasia. Bratisl Lek Listy. 2008; 109(11):528–530. PMID: 19205567.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Persistent Aneurysm Growth Following Pipeline Embolization Device Assisted Coiling of a Fusiform Vertebral Artery Aneurysm: A Word of Caution!
- Treatment for Giant Fusiform Aneurysm Located in the Cavernous Segment of the Internal Carotid Artery Using the Pipeline Embolization Device
- Inadvertent Complication of a Pipeline Embolization Device for Treatment with Vertebral Artery Dissecting Aneurysm : Distal Tip Fracture of Delivery Wire
- A Case of Ruptured Blood Blister-like Aneurysm Treated with Pipeline Embolization Device: Clinical Significance of Fetal-type Posterior Communicating Artery
- Microsurgical Strategies Following Failed Endovascular Treatment with the Pipeline Embolization Device: Case of a Giant Posterior Cerebral Artery Aneurysm
