Ann Dermatol.
2011 Aug;23(3):357-361. 10.5021/ad.2011.23.3.357.
Treatment of Keratoacanthoma with 5% Imiquimod Cream and Review of the Previous Report
- Affiliations
-
- 1Department of Dermatology, Seoul National University College of Medicine, Seoul, Korea. khcho@snu.ac.kr
- KMID: 2171929
- DOI: http://doi.org/10.5021/ad.2011.23.3.357
Abstract
- Keratoacanthoma (KA) is a benign epidermal tumor, characterized by rapid and abundant growth, a tendency toward spontaneous regression and histopathologic similarity to squamous cell carcinoma (SCC). Because KA can be easily misdiagnosed as SCC, surgery is considered the treatment of choice. Recently, regression of KAs following application of 5% imiquimod cream (Aldara(R)) has been reported. We present 4 cases of KA treated with topical imiquimod, applied 3 to 4 times a week. Obvious improvement was observed after 4 to 6 weeks of application and the lesions were almost cleared leaving scars after 9 to 11 weeks. These results show that topical imiquimod can be an effective option for the conservative management of KA as previously reported. We also suggest that lesions treated with imiquimod cream should be considered for biopsy to judge histopathological remission after 5 to 8 weeks of application to shorten the duration of the treatment.
Keyword
Figure
-
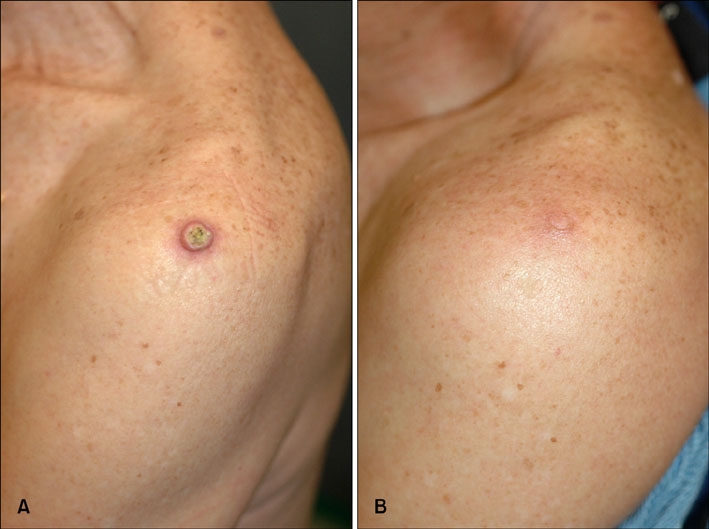
Fig. 1 (A) The lesion of case 1 on the left shoulder before therapy. (B) The lesion regressed completely after 11 weeks.

Fig. 2 (A) The lesion of case 2 before therapy. (B) The lesion regressed completely after 10 weeks.
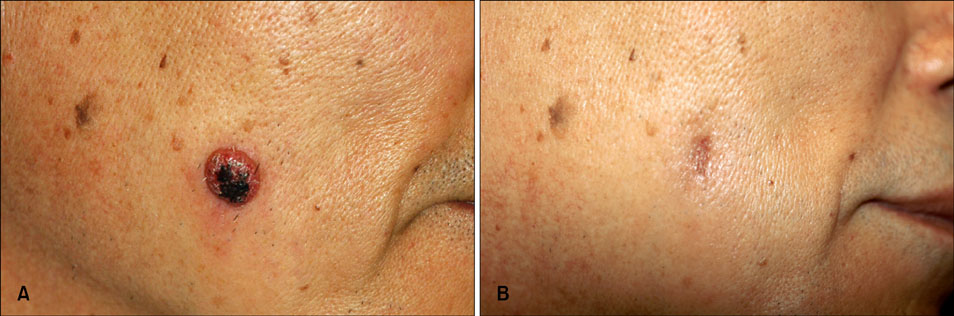
Fig. 3 (A) The lesion of case 3 on the right cheek before therapy. (B) The lesion regressed completely after 13 weeks.
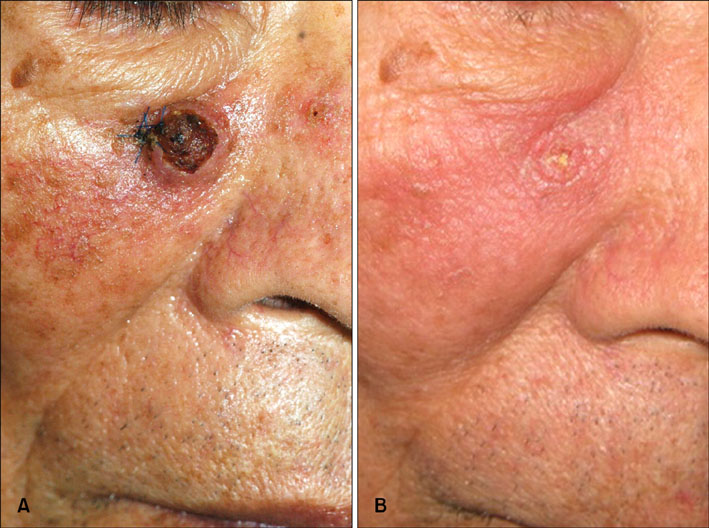
Fig. 4 (A) The lesion of case 4 before therapy. (B) The lesion regressed completely after 12 weeks.
Reference
-
1. Karaa A, Khachemoune A. Keratoacanthoma: a tumor in search of a classification. Int J Dermatol. 2007. 46:671–678.
Article2. Beham A, Regauer S, Soyer HP, Beham-Schmid C. Keratoacanthoma: a clinically distinct variant of well differentiated squamous cell carcinoma. Adv Anat Pathol. 1998. 5:269–280.3. Kwittken J. A histologic chronology of the clinical course of the keratocarcinoma (so-called keratoacanthoma). Mt Sinai J Med. 1975. 42:127–135.4. Griffiths RW. Keratoacanthoma observed. Br J Plast Surg. 2004. 57:485–501.
Article5. Seifert A, Nasemann T. Keratoacanthoma and its clinical variants. Review of the literature and histopathologic analysis of 90 cases. Hautarzt. 1989. 40:189–202.6. Yoshikawa K, Katagata Y, Kondo S. Relative amounts of keratin 17 are higher than those of keratin 16 in hair-follicle-derived tumors in comparison with nonfollicular epithelial skin tumors. J Invest Dermatol. 1995. 104:396–400.
Article7. Schwartz RA. Keratoacanthoma: a clinico-pathologic enigma. Dermatol Surg. 2004. 30:326–333.
Article8. Yuge S, Godoy DA, Melo MC, Sousa DS, Soares CT. Keratoacanthoma centrifugum marginatum: response to topical 5-fluorouracil. J Am Acad Dermatol. 2006. 54:5 Suppl. S218–S219.
Article9. Vergara A, Isarría MJ, Domínguez JD, Gamo R, Rodríguez Peralto JL, Guerra A. Multiple and relapsing keratoacanthomas developing at the edge of the skin grafts site after surgery and after radiotherapy. Dermatol Surg. 2007. 33:994–996.
Article10. Annest NM, VanBeek MJ, Arpey CJ, Whitaker DC. Intralesional methotrexate treatment for keratoacanthoma tumors: a retrospective study and review of the literature. J Am Acad Dermatol. 2007. 56:989–993.
Article11. Dendorfer M, Oppel T, Wollenberg A, Prinz JC. Topical treatment with imiquimod may induce regression of facial keratoacanthoma. Eur J Dermatol. 2003. 13:80–82.12. Bhatia N. Imiquimod as a possible treatment for keratoacanthoma. J Drugs Dermatol. 2004. 3:71–74.13. Di Lernia V, Ricci C, Albertini G. Spontaneous regression of keratoacanthoma can be promoted by topical treatment with imiquimod cream. J Eur Acad Dermatol Venereol. 2004. 18:626–629.
Article14. Kim YJ, Hwang ES, Son SW, Kim IH. Topical treatment with 5% imiquimod for solitary keratoacanthoma. Korean J Dermatol. 2004. 42:1321–1324.15. Ko NY, Park JH, Son SW, Kim IH. Treatment of keratoacanthoma with 5% imiquimod cream. Ann Dermatol. 2006. 18:14–17.
Article16. Calista D, Morri M. Topical imiquimod for the treatment of keratoacanthomas. Eur J Dermatol. 2008. 18:590–591.17. Paternò EJ, Campione E, Diluvio L, Orlandi A, Chimenti S. Imiquimod for restoring local immunity in a renal transplant patient with persistent keratoacanthoma. Dermatol Online J. 2008. 14:8.
Article
