A Family Presenting with Catastrophic Features due to Pheochromocytoma Associated with Multiple Endocrine Neoplasia 2A
- Affiliations
-
- 1Department of Endocrinology and Metabolism, Kyung Hee University School of Medicine, Seoul, Korea. jtwoomd@khmc.or.kr
- 2Endocrine Research Institute, Kyung Hee University School of Medicine, Seoul, Korea.
- 3Department of Nephrology, Kyung Hee University School of Medicine, Seoul, Korea.
- 4Department of Internal Medicine, Dong Su Won General Hospital, Suwon, Korea.
- KMID: 2169020
- DOI: http://doi.org/10.3803/EnM.2010.25.2.135
Abstract
- Multiple endocrine neoplasia 2A (MEN 2A) is an autosomal dominant disease that consists of medullary thyroid carcinoma (MTC), pheochromocytoma and parathyroid hyperplasia. The activation of germ-line mutations in the RET proto-oncogene are responsible for MEN 2A. We describe here a rare case of MEN 2A in a patient who presented with an acute catecholamine-induced cardiomyopathy with cardiogenic shock and acute renal failure. The patient was diagnosed with pheochromocytoma and MTC associated with MEN 2A, which was confirmed by the detection of a RET proto-oncogene mutation at exon 11 on codon 634 (Cys634Arg). During familial screening, the patient's younger sister was found to have a benign thyroid nodule. Re-evaluation of this thyroid nodule revealed MTC with the same gene mutation. We also provide a review of the relevant literature.
MeSH Terms
Figure
-

Fig. 1 Left adrenal mass. A. Adrenal MRI (T2 weighted image) showed 2.9 × 3.3 × 4.9 cm-sized heterogeneous high signal intensity mass with internal cystic changes in the left adrenal gland. B. 131I-MIBG scan showed increased radioactivity in the left adrenal gland.
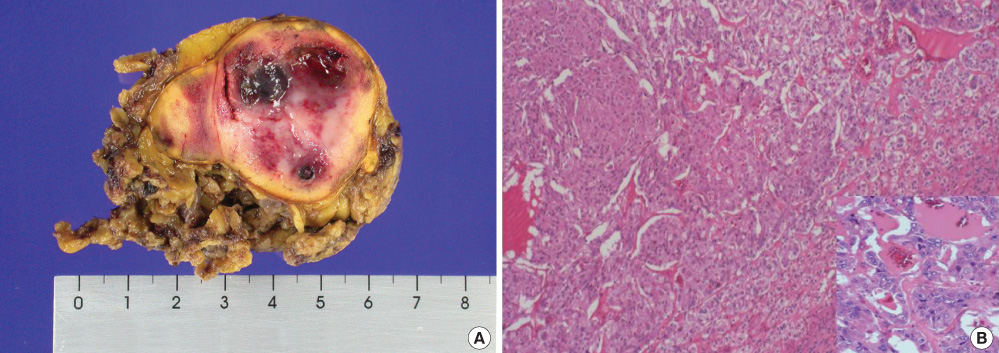
Fig. 2 Histology of the resected adrenal gland. A. Left adrenal gland specimen, in which a 5 × 4 cm-sized mass was noted. The cut surface showed a rather well-demarcated golden yellow/brown nodular mass with hemorrhage. B. Microscopic finding of pheochromocytoma showed that the area was largely replaced by tumor tissue consisting of clusters or nests or glands of neoplastic cells (H&E stain, × 100, × 400 [in bottom right]).
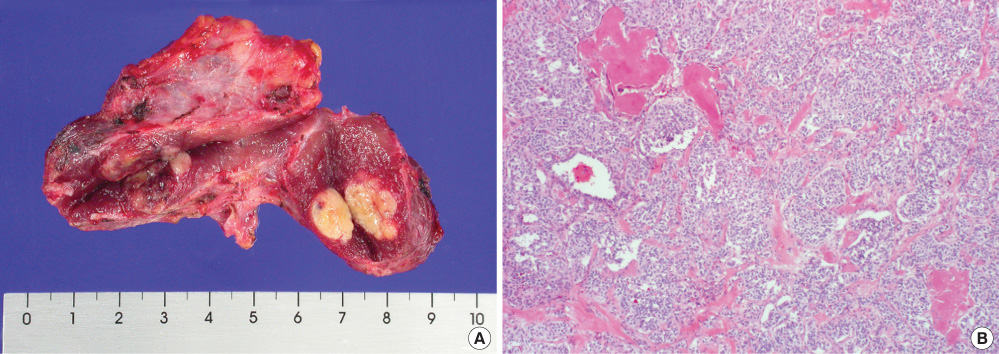
Fig. 3 Histology of the resected thyroid gland. A. Total thyroidectomy specimen was measured to be 9 × 5 cm in size and 25 g in weight. A cut section showed multiple yellow/brown variable-sized nodules. The left thyroid showed a well-defined yellowish mass measuring 1.5 × 1 cm. The right thyroid showed a well-demarcated dark brown mass measuring 2 × 1.5 cm. B. Microscopic finding of medullary thyroid carcinoma showed multiple rather well-defined tumor nodules consisting of nests or clusters of tumor cells with dense fibrous to hyalinized stroma (H&E stain, × 100).
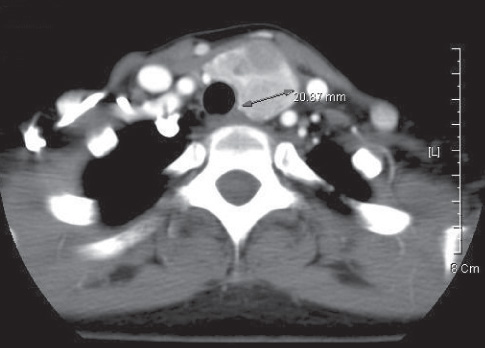
Fig. 4 Neck CT of the thyroid nodule in the younger sister of the patient. Diffuse enlargement of the thyroid gland and multiple nodules of various sizes were observed. The largest solid mass was 2.1 cm in size and was found in the left thyroid gland. No abnormal lymph nodes were observed.

Fig. 5 Histology of the resected thyroid gland in younger sister of the patient. A. The total thyroidectomy specimen measured 34 g. The left thyroid was 5 × 3 × 3 cm in size, and a cut surface showed multinodular gray/white masses measuring 4 × 3 cm. The right thyroid was 3 × 3 × 2 cm in size, and a cut surface showed a gray/white nodular mass measuring 1.5 × 1 cm. B. Microscopic findings of the thyroid medullary carcinoma showed ill-defined tumor tissue consisting of proliferating round to polygonal cells with granular amphophilic cytoplasm and medium-sized nuclei separated by a vascular stroma, hyalinized collagen, and amyloid tissue arranged in a follicular and trabecular pattern. Associated calcification was evident (H&E stain, × 100).

Fig. 6 Direct sequence analysis of exon 11 of the RET gene and the resulting family tree. The analysis shows family members (patient, younger sister of patient) with a mutation at exon 11, codon 634 (C634R), TGC (Cysteine) → CGC (Arginine). A. Wild type, B. Mutant type, C. Pedigree of the patient.
Reference
-
1. Mulligan LM, Kwok JB, Healey CS, Elsdon MJ, Eng C, Gardner E, Love DR, Mole SE, Moore JK, Papi L, Ponder MA, Telenius H, Tunnacliffe A, Ponder BJ. Germ-line mutations of the RET proto-oncogene in multiple endocrine neoplasia type 2A. Nature. 1993. 363:458–460.2. Lindskog S, Nilsson O, Jansson S, Nilsson B, Illerskog AC, Ysander L, Ahlman H, Tisell LE. Phenotypic expression of a family with multiple endocrine neoplasia type 2A due to a RET mutation at codon 618. Br J Surg. 2004. 91:713–718.3. Rodriguez JM, Balsalobre M, Ponce JL, Rios A, Torregrosa NM, Tebar J, Parrilla P. Pheochromocytoma in MEN 2A syndrome. Study of 54 patients. World J Surg. 2008. 32:2520–2526.4. Quayle FJ, Fialkowski EA, Benveniste R, Moley JF. Pheochromocytoma penetrance varies by RET mutation in MEN 2A. Surgery. 2007. 142:800–805.5. Kim J, Reutrakul S, Davis DB, Kaplan EL, Refetoff S. Multiple endocrine neoplasia 2A syndrome presenting as peripartum cardiomyopathy due to catecholamine excess. Eur J Endocrinol. 2004. 151:771–777.6. Brandi ML, Gagel RF, Angeli A, Bilezikian JP, Beck-Peccoz P, Bordi C, Conte-Devolx B, Falchetti A, Gheri RG, Libroia A, Lips CJ, Lombardi G, Mannelli M, Pacini F, Ponder BA, Raue F, Skogseid B, Tamburrano G, Thakker RV, Thompson NW, Tomassetti P, Tonelli F, Wells SA Jr, Marx SJ. Guidelines for diagnosis and therapy of MEN type 1 and type 2. J Clin Endocrinol Metab. 2001. 86:5658–5671.7. Karagiannis A, Mikhailidis DP, Athyros VG, Harsoulis F. Pheochromocytoma: an update on genetics and management. Endocr Relat Cancer. 2007. 14:935–956.8. Suh IW, Lee CW, Kim YH, Hong MK, Lee JW, Kim JJ, Park SW, Park SJ. Catastrophic catecholamine-induced cardiomyopathy mimicking acute myocardial infarction, rescued by extracorporeal membrane oxygenation (ECMO) in pheochromocytoma. J Korean Med Sci. 2008. 23:350–354.9. Liao WB, Liu CF, Chiang CW, Kung CT, Lee CW. Cardiovascular manifestations of pheochromocytoma. Am J Emerg Med. 2000. 18:622–625.10. Nirgiotis JG, Andrassy RJ. Pheochromocytoma and acute myocardial infarction. South Med J. 1990. 83:1478–1480.11. Takabatake T, Kawabata M, Ohta H, Yamamoto Y, Ishida Y, Hara H, Hattori N. Acute renal failure and transient, massive proteinuria in a case of pheochromocytoma. Clin Nephrol. 1985. 24:47–49.12. Eisenhofer G, Walther MM, Huynh TT, Li ST, Bornstein SR, Vortmeyer A, Mannelli M, Goldstein DS, Linehan WM, Lenders JW, Pacak K. Pheochromocytomas in von Hippel-Lindau syndrome and multiple endocrine neoplasia type 2 display distinct biochemical and clinical phenotypes. J Clin Endocrinol Metab. 2001. 86:1999–2008.13. Kaltsas GA, Papadogias D, Grossman AB. The clinical presentation (symptoms and signs) of sporadic and familial chromaffin cell tumours (phaeochromocytomas and paragangliomas). Front Horm Res. 2004. 31:61–75.14. Yun SW, Yoo WS, Hong KH, Kim BH, Kang MH, Choo YK, Park HY, Kim DH, Chung HK, Chang MC, Kwon MS, Kim HJ. A family of multiple endocrine neoplasia type 2A with a C634R mutation and a G691S polymorphism in RET proto-oncogene. J Korean Soc Endocrinol. 2007. 22:453–459.15. Yang HY, Park YJ, Kwon HJ, Choe KJ. Cermline mutation of RET gene in a multiple endocrine neoplasia type 2A (MEN2A) family. J Korean Cancer Assoc. 1999. 31:867–875.16. Yang JH, Woo SW. The characteristics of multiple endocrine neoplasia in Korean. Korean J Endocr Surg. 2005. 5:1–6.17. Kim HH, Kim HJ, Chung YJ, Min YK, Lee MS, Lee MK, Kim KW, Ki CS, Kim JW, Chung JH. Analysis of ret proto-oncogene mutation in Korean patients with medullary thyroid carcinomas. J Korean Soc Endocrinol. 2003. 18:360–370.18. Schuffenecker I, Virally-Monod M, Brohet R, Goldgar D, Conte-Devolx B, Leclerc L, Chabre O, Boneu A, Caron J, Houdent C, Modigliani E, Rohmer V, Schlumberger M, Eng C, Guillausseau PJ, Lenoir GM. Groupe D'etude des Tumeurs à Calcitonine. Risk and penetrance of primary hyperparathyroidism in multiple endocrine neoplasia type 2A families with mutations at codon 634 of the RET proto-oncogene. J Clin Endocrinol Metab. 1998. 83:487–491.19. Renshaw AA. Accuracy of thyroid fine-needle aspiration using receiver operator characteristic curves. Am J Clin Pathol. 2001. 116:477–482.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ectopic ACTH Syndrome with Bilateral Pheochromocytoma in Multiple Endocrine Neoplasia Type 2A
- A family of multiple endocrine neoplasia type 2A associated with a C618R mutation in RET proto-oncogene
- A Case of Insulinoma Combined with Pheochromocytoma
- A Case of Multiple endocrine neoplasia type 2a
- Multiple Endocrine Neoplasia 2A Detected by Peptic Ulcer Perforation with Hypercalcemia
