Imaging findings in a case of Gorlin-Goltz syndrome: a survey using advanced modalities
- Affiliations
-
- 1Oral Radiology Department, Dental School, Shiraz University of Medical Sciences, Shiraz, Iran. pegah_brix@yahoo.com
- 2TABA Medical Imaging Center, Shiraz, Iran.
- 3Oral Pathology Department, Babol Dental School, Babol, Iran.
- KMID: 2167403
- DOI: http://doi.org/10.5624/isd.2011.41.4.171
Abstract
- Gorlin-Goltz syndrome is an infrequent multi-systemic disease which is characterized by multiple keratocysts in the jaws, calcification of falx cerebri, and basal cell carcinomas. We report a case of Gorlin-Goltz syndrome in a 23-year-old man with emphasis on image findings of keratocyctic odontogenic tumors (KCOTs) on panoramic radiograph, computed tomography, magnetic resonance (MR) imaging, and Ultrasonography (US). In this case, pericoronal lesions were mostly orthokeratinized odontogenic cyst (OOC) concerning the MR and US study, which tended to recur less. The aim of this report was to clarify the characteristic imaging features of the syndrome-related keratocysts that can be used to differentiate KCOT from OOC. Also, our findings suggested that the recurrence rate of KCOTs might be predicted based on their association to teeth.
Keyword
MeSH Terms
Figure
-

Fig. 1 Panoramic radiograph shows multiple cystic odontogenic lesions in both jaws.

Fig. 2 Skull PA radiograph shows falx cerebri calcification.
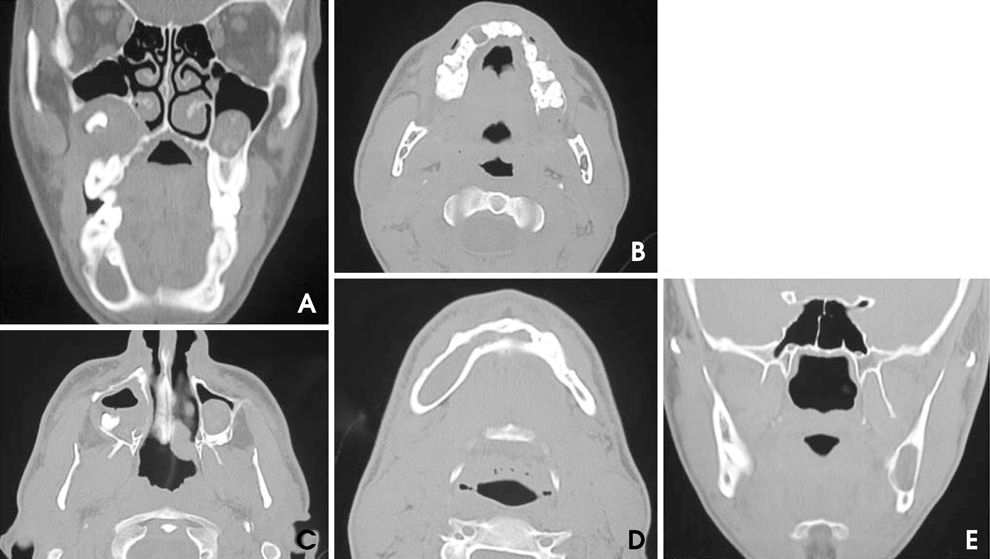
Fig. 3 A. Coronal CT scan shows a cystic lesion associated with an impact tooth causing expansion and displacement of the floor of the right antrum and a mucous retention cyst in the left sinus. B. Axial CT scan shows a lytic lesion in the region of right maxillary canine as well as in ramus both sides. C. Axial CT scan shows soft tissue density in the right maxillary sinus with mucoperiosteal thickening and thinning of medial wall. D. Axial CT scan of the mandible reveals a well defined expansile lytic lesion in the right side crossing midline. E. Coronal CT scan shows a hypodense expansile lesion causing thinning of medial wall of the left mandibular ramus.
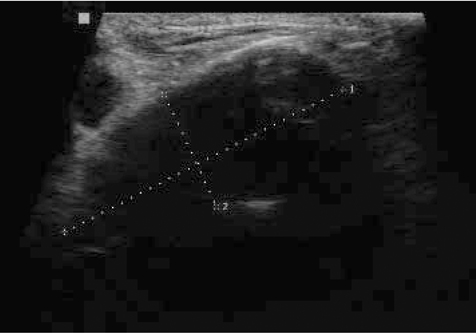
Fig. 4 Ultrasonograph shows a well demarcated hypoechoic lesions in the right side of mandible.
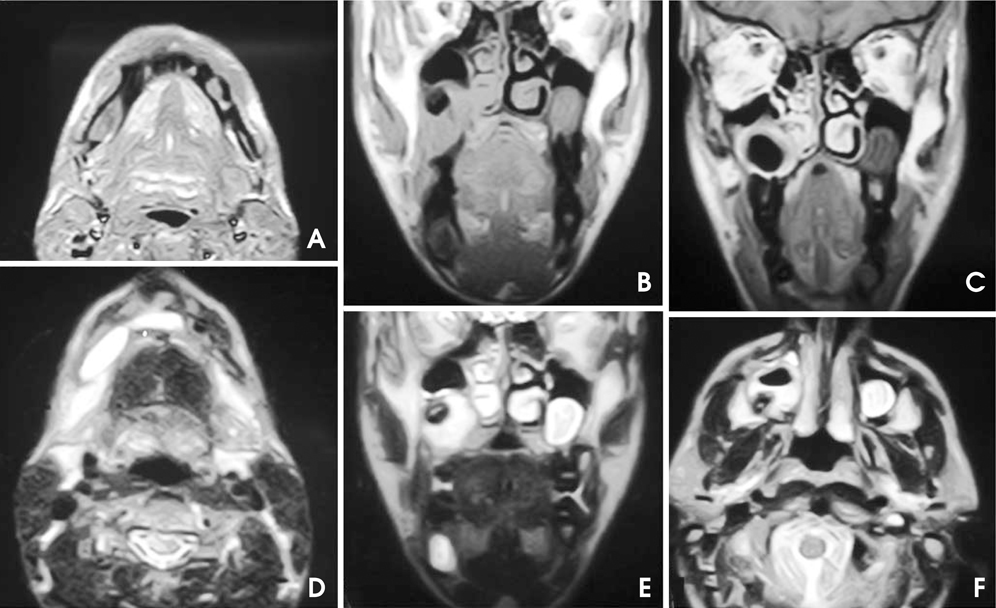
Fig. 5 A. Axial T1WI of mandible shows intermediate signal intensity (SI). B. Coronal T1W MRI of patient shows an expansion of inferior wall of the right maxillary sinus and anterior wall of nasal cavity due to low-intermediate SI lesion associated with an impacted tooth (signal void). C. Coronal post contrast T1W MRI reveals moderate enhancement of cystic wall in the right maxillary sinus. D. Axial T2WI of the mandible shows a homogenous high SI lesion. E. Coronal T2W MRI reveals a well defined expansile hyperintense lesion inferior to the right antrum with heterogeneous signal intensity. F. Axial T2WI of the maxilla shows a hyper intense heterogeneous lesion and a retention pseudocyst.
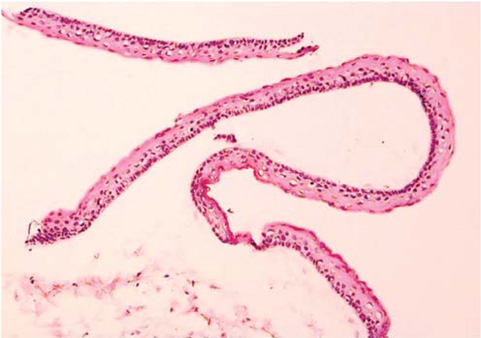
Fig. 6 Histopathologic view of KCOT (H&E stain, ×10). The epithelial lining is 6 to 8 cells thick, with a hyperchromatic and palisaded basal cell layer. Note the corrugated parakeratotic surface.
Reference
-
1. Jones EA, Sajid MI, Shenton A, Evans DG. Basal cell carcinomas in gorlin syndrome: a review of 202 patients. J Skin Cancer. 2011. 2011:217378.
Article2. Kantarci M, Ertas U, Alper F, Sutbeyaz Y, Karasen RM, Onbas O. Gorlin's syndrome with a thin corpus callosum and a third ventricular cyst. Neuroradiology. 2003. 45:390–392.
Article3. Kalogeropoulou C, Zampakis P, Kazantzi S, Kraniotis P, Mastronikolis NS. Gorlin-Goltz syndrome: incidental finding on routine CT scan following car accident. Cases J. 2009. 2:9087.
Article4. White SC, Pharoah MJ. Oral radiology principles and interpretation. 2009. 6th ed. St. Louis: Mosby Elsevier;351.5. Ariji Y, Morita M, Katsumata A, Sugita Y, Naitoh M, Goto M, et al. Imaging features contributing to the diagnosis of ameloblastomas and keratocyctic odontogenic tumours: logistic regression analysis. Dentomaxillofac Radiol. 2011. 40:133–140.6. Minami M, Kaneda T, Ozawa K, Yamamoto H, Itai Y, Ozawa M, et al. Cystic lesions of the maxillomandibular region: MR imaging distinction of odontogenic keratocysts and ameloblastomas from other cysts. AJR Am J Roentgenol. 1996. 166:943–949.
Article7. Hisatomi M, Asaumi J, Konouchi H, Shigehara H, Yanagi Y, Kishi K. MR imaging of epithelial cysts of the oral and maxillofacial region. Eur J Radiol. 2003. 48:178–182.
Article8. Kaneda T. MR imaging of maxillomandibular lesions. Oral Radiol. 2003. 19:64–69.
Article9. Ortega García de Amezaga A, García Arregui O, Zepeda Nuño S, Acha Sagredo A, Aguirre Urizar JM. Gorlin-Goltz syndrome: clinicopathologic aspects. Med Oral Patol Oral Cir Bucal. 2008. 13:E338–E343.10. Lauria L, Curi MM, Chammas MC, Pinto DS, Torloni H. Ultrasonography evaluation of bone lesions of the jaw. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996. 82:351–357.11. Bagewadi SB, VG M, Patil K. Ultrasonography of swellings in orofacial region. J Indian Acad Oral Med Radiol. 2010. 22:18–26.12. Sumer AP, Danaci M, Ozen Sandikçi E, Sumer M, Celenk P. Ultrasonography and Doppler ultrasonography in the evaluation of intraosseous lesions of the jaws. Dentomaxillofac Radiol. 2009. 38:23–27.
Article13. Macdonald-Jankowski DS. Orthokeratinized odontogenic cyst: a systemic review. Dentomaxillofac Radiol. 2010. 39:455–467.14. Philipsen HP. Barnes L, Eveson JW, Reichart P, Sidransky D. Keratocystic odontogenic tumour. World Health Organization classification of tumours. Pathology and genetics of head and neck tumours. 2005. Lyon: IARC;306–307.15. Bolbaran V, Martinez B, Rojas R. Odontogenic keratocysts. A retrospective study of 285 cases (I. Clinical aspects). Med Oral. 2000. 5:331–337.16. Bolbaran V, Martinez B, Rojas R. Odontogenic keratocysts. A retrospective study of 285 cases (II. Histopathological aspects). Med Oral. 2000. 5:338–344.17. MacDonald-Jankowski DS. Keratocystic odontogenic tumour: systemic review. Dentomaxillofac Radiol. 2011. 40:1–23.18. Crowley TE, Kaugars GE, Gunsolley JC. Odontogenic keratocysts: a clinical and histologic comparison of the parakeratin and orthokeratin variants. J Oral Maxillofac Surg. 1992. 50:22–26.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The First Korean Case of Gorlin?Goltz Syndrome Caused by a PTCH2 Pathogenic Variant Identified via Whole Exome Sequencing
- Radiological features of familial Gorlin-Goltz syndrome
- Novel Patched 1 Mutations in Patients with Gorlin-Goltz Syndrome Strategic Treated by Smoothened Inhibitor
- Basal cell nevus syndrome with excessive basal cell carcinomas
- Goltz Syndrome Associated with Omphalocele
