Radiological features of familial Gorlin-Goltz syndrome
- Affiliations
-
- 1Department of Oral Medicine and Radiology, AB Shetty Memorial Institute of Dental Sciences, Nitte University, Mangalore, India. drshruthihegde@yahoo.co.in
- KMID: 1974408
- DOI: http://doi.org/10.5624/isd.2012.42.1.55
Abstract
- Gorlin-Goltz syndrome is an autosomal dominant disorder principally characterized by cutaneous basal cell carcinomas, multiple keratocystic odontogenic tumors, and skeletal anomalies. This syndrome may be diagnosed early by dentist because keratocystic odontogenic tumors are usually one of the first manifestations of the syndrome. Early diagnosis and treatment are of utmost importance in reducing the severity of long term sequelae of this syndrome. This report presents a rare event of Gorlin-Goltz syndrome occurring in a 39-year-old male and his 8-year-old daughter. The clinical and investigative features of this familial disorder has been described in detail.
MeSH Terms
Figure
-

Fig. 1 A. Photograph shows increased inner canthal distance. B. Cystic swelling on the left eyelid is seen. C. Cystic swelling in the midline of the neck is seen.

Fig. 2 Panoramic radiograph shows multiple unilocular radiolucencies in mandibular body, ramus, and symphysis region and a smaller unilocular radiolucency in the right maxillary tuberosity area.
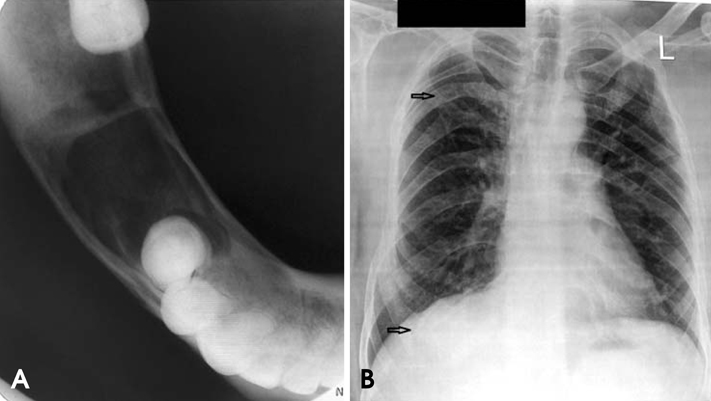
Fig. 3 A. The mandibular occlusal cross sectional radiograph shows a radiolucent area with minimum cortical plate expansion. B. The chest radiograph shows bifid fourth and eighth rib on the right side.

Fig. 4 A. Axial CT image shows hypodense areas in relation to the right mandibular body separated by hyperdense septae. B. Coronal CT image shows the lesion involving the right half of maxilla including maxillary sinus. C. Axial CT image shows calcification of falx cerebri.
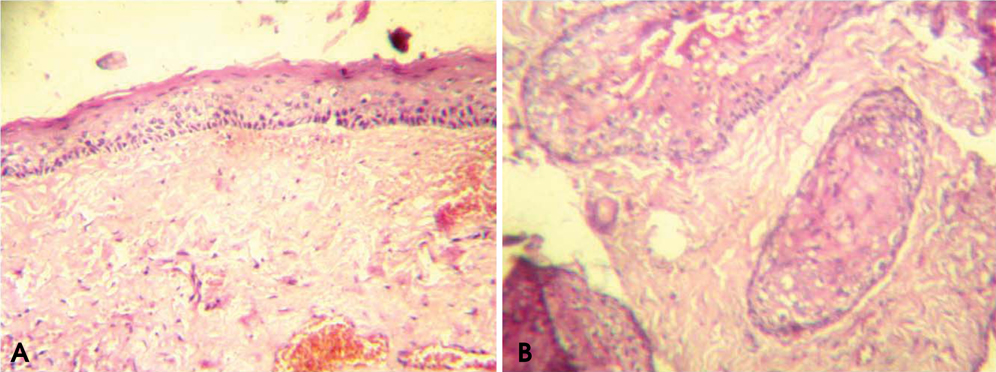
Fig. 5 Photomicrographs show the parakeratinized, corrugated, 6-10 layers thick epithelium with palisaded, polarized basal cell layer. Also, daughter cysts in connective tissue suggestive of an keratocystic odontogenic tumor is observed (H&E stain, A. ×40, B. ×100) .
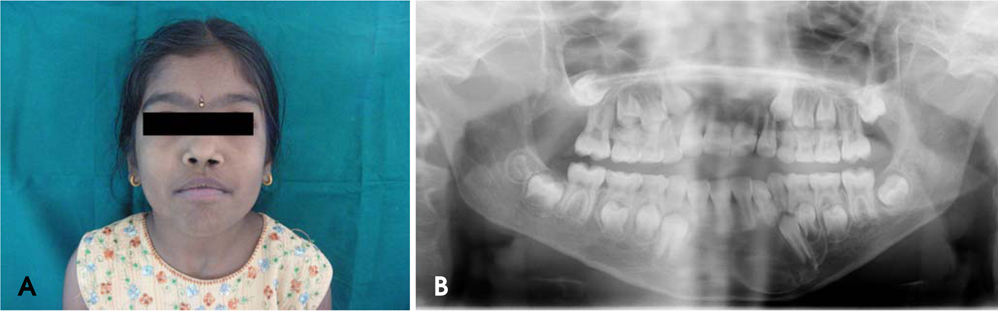
Fig. 6 A. The daughter's photograph reveals hypertelorism. B. Her panoramic radiograph shows well defined radiolucency in the mandibular symphysis region with displacement of the erupting canine.
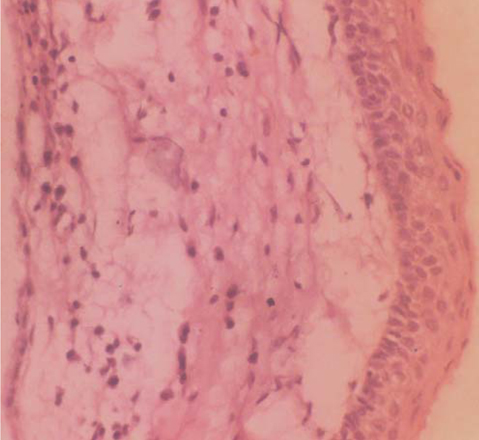
Fig. 7 Photomicrograph shows the parakeratinized, corrugated, 6-8 layers thick epithelium with palisaded, polarized basal cell layer (H&E stain, ×100).
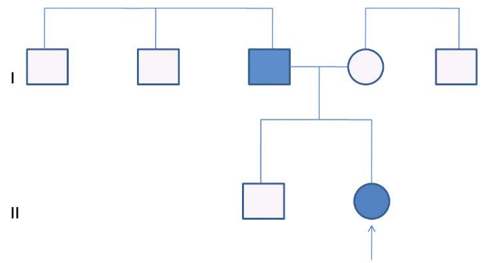
Fig. 8 Pedigree chart of the affected family shows the mode of inheritance of Gorlin-Goltz syndrome.
Cited by 1 articles
-
Bilateral inflammatory cysts of the jaw: report of an unusual case
Vidya A. Holla, Laxmikanth Chatra, Prashanth Shenai, Prasanna Kumar Rao, KM Veena, Rachana Vishnudas Prabhu
Imaging Sci Dent. 2012;42(2):105-109. doi: 10.5624/isd.2012.42.2.105.
Reference
-
1. Gorlin RJ, Goltz RW. Multiple nevoid basal-cell epithelioma, jaw cysts and bifid rib. A syndrome. N Engl J Med. 1960. 262:908–912.2. Manfredi M, Vescovi P, Bonanini M, Porter S. Nevoid basal cell carcinoma syndrome: a review of the literature. Int J Oral Maxillofac Surg. 2004. 33:117–124.
Article3. Casaroto AR, Loures DC, Moreschi E, Veltrini VC, Trento CL, Gottardo VD, et al. Early diagnosis of Gorlin-Goltz syndrome: case report. Head Face Med. 2011. 7:2.
Article4. Markt JC. Implant prosthodontic rehabilitation of a patient with nevoid basal cell carcinoma syndrome: a clinical report. J Prosthet Dent. 2003. 89:436–442.
Article5. Honavar SG, Shields JA, Shields CL, Eagle RC, Demirci H, Mahmood EZ. Basal cell carcinoma of the eyelid associated with Gorlin-Goltz syndrome. Ophthalmology. 2001. 108:1115–1123.6. Doede T, Seidel J, Riede FT, Vogt L, Mohr FW, Schier F. Occult, life-threatening, cardial tumor in syndactylism in Gorlin Goltz syndrome. J Pediatr Surg. 2004. 39:e17–e19.
Article7. Deepa MS, Paul R, Balan A. Gorlin Goltz syndrome: a review. J Indian Acad Oral Med Radiol. 2003. 15:203–209.8. Lo Muzio L, Nocini P, Bucci P, Pannone G, Consolo U, Procaccini M. Early diagnosis of nevoid basal cell carcinoma syndrome. J Am Dent Assoc. 1999. 130:669–674.9. Melo ES, Kawamura JY, Alves CA, Nunes FD, Jorge WA, Cavalcanti MG. Imaging modality correlations of an odontogenic keratocyst in the nevoid basal cell carcinoma syndrome: a family case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004. 98:232–236.
Article10. Lee BD, Kim JH, Choi DH, Koh KS, Lee SR. Recurrent odontogenic keratocysts in basal cell nevus syndrome: report of a case. Korean J Oral Maxillofac Radiol. 2004. 34:203–207.11. Kimonis VE, Goldstein AM, Pastakia B, Yang ML, Kase R, DiGiovanna JJ, et al. Clinical manifestations in 105 persons with nevoid basal cell carcinoma syndrome. Am J Med Genet. 1997. 69:299–308.
Article12. Gorlin RJ, Cohen MM, Levin LS. Syndromes of the head and neck. 1990. 3rd ed. New York: Oxford University Press;372–378.13. Jarish W. Zur lehre von den autgeschwulsten. Archiv Jur Dermatologic Syphilogic. 1894. 28:163–222.14. Patil K, Mahima VG, Gupta B. Gorlin syndrome: a case report. J Indian Soc Pedod Prev Dent. 2005. 23:198–203.
Article15. Rai S, Gauba K. Jaw cyst-Basal cell nevus-Bifid rib syndrome: a case report. J Indian Soc Pedod Prev Dent. 2007. 25:137–139.
Article16. Jones EA, Sajid MI, Shenton A, Evans DG. Basal cell carcinomas in gorlin syndrome: a review of 202 patients. J Skin Cancer. 2011. 2011:217378.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The First Korean Case of Gorlin?Goltz Syndrome Caused by a PTCH2 Pathogenic Variant Identified via Whole Exome Sequencing
- Imaging findings in a case of Gorlin-Goltz syndrome: a survey using advanced modalities
- Multidisciplinary approach to Gorlin-Goltz syndrome: from diagnosis to surgical treatment of jawbones
- Basal cell nevus syndrome with excessive basal cell carcinomas
- Novel Patched 1 Mutations in Patients with Gorlin-Goltz Syndrome Strategic Treated by Smoothened Inhibitor
