Experience of direct percutaneous sac injection in type II endoleak using cone beam computed tomography
- Affiliations
-
- 1Division of Vascular Surgery, Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. dikim@skku.edu
- 2Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2167025
- DOI: http://doi.org/10.4174/astr.2015.88.4.232
Abstract
- Cone beam CT, usually used in dental area, could easily obtain 3-dimensional images using cone beam shaped ionized radiation. Cone beam CT is very useful for direct percutaneous sac injection (DPSI) which needs very precise measurement to avoid puncture of inferior vena cava or vessel around sac or stent graft. Here we describe two cases of DPSI using cone beam CT. In case 1, a 79-year-old male had widening of preexisted type II endoleak after endovascular aneurysm repair (EVAR). However, transarterial embolization failed due to tortuous collateral branches of lumbar arteries. In case 2, a 72-year-old female had symptomatic sac enlargement by type II endoleak after EVAR. However, there was no route to approach the lumbar arteries. Therefore, we performed DPSI assisted by cone beam CT in cases 1, 2. Six-month CT follow-up revealed no sign of sac enlargement by type II endoleak.
MeSH Terms
Figure
-
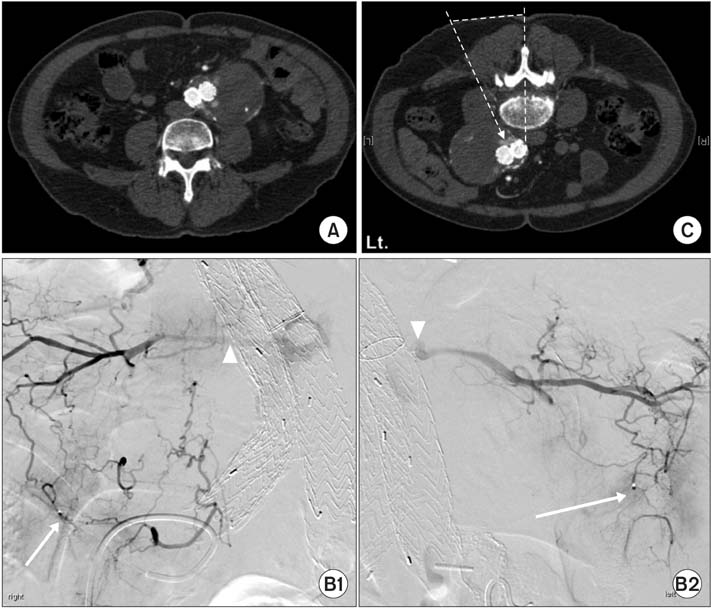
Fig. 1 (A) Type II endoleak. (B) Transarterial approach was failed due to tortuous collateral branches of both lumbar arteries. The tip of a microcatheter in a collateral branch from the internal iliac artery (white arrows), the lumbar artery reconstituted from a collateral branch from the internal iliac artery (white arrow heads). (C) Direction of direct percutaneous sac injection. The patient was placed in prone position. 21-gauge Chiba needle was inserted through paraspinal route directly into type II endoleak sac under fluoroscopy guidance.
Fig. 2 (A) Type II endoleak. (B) Transarterial approach was failed due to tortuous collateral branches of lumbar arteries. A tortuous collateral artery from the internal iliac artery (white arrow). (C) Direction of direct percutaneous sac injection using cone beam CT. (D) Two milliliters of glue mixed in 4 mL of Lipidol was injected into the type II endoleak sac under fluoroscopy guidance.
Reference
-
1. Gelfand DV, White GH, Wilson SE. Clinical significance of type II endoleak after endovascular repair of abdominal aortic aneurysm. Ann Vasc Surg. 2006; 20:69–74.2. Uthoff H, Katzen BT, Gandhi R, Pena CS, Benenati JF, Geisbusch P. Direct percutaneous sac injection for postoperative endoleak treatment after endovascular aortic aneurysm repair. J Vasc Surg. 2012; 56:965–972.3. De Vos W, Casselman J, Swennen GR. Cone-beam computerized tomography (CBCT) imaging of the oral and maxillofacial region: a systematic review of the literature. Int J Oral Maxillofac Surg. 2009; 38:609–625.4. Feldkamp LA, Davis LC, Kress JW. Practical cone-beam algorithm. J Opt Soc Am A. 1984; 1:612–619.5. Larson BE. Cone-beam computed tomography is the imaging technique of choice for comprehensive orthodontic assessment. Am J Orthod Dentofacial Orthop. 2012; 141:402.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Management of root canal perforation by using cone-beam computed tomography
- Three-dimensional imaging modalities in endodontics
- Detection of maxillary second molar with two palatal roots using cone beam computed tomography: a case report
- Cone beam computed tomography findings of ectopic mandibular third molar in the mandibular condyle: report of a case
- Endovascular Treatment of Type II Endoleak Following Thoracic Endovascular Aortic Repair for Thoracic Aortic Aneurysm: Case Report of Squeeze Technique to Reach the Aneurysmal Sac
