Ann Surg Treat Res.
2016 Feb;90(2):64-71. 10.4174/astr.2016.90.2.64.
A simple pancreaticojejunostomy technique for hard pancreases using only two transpancreatic sutures with buttresses: a comparison with the previous pancreaticogastrostomy and dunking methods
- Affiliations
-
- 1Department of Hepatobiliary and Pancreas Surgery, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. gshth@catholic.ac.kr
- KMID: 2166824
- DOI: http://doi.org/10.4174/astr.2016.90.2.64
Abstract
- PURPOSE
In this study, we introduced a novel technique, the pancreaticojejunostomy (PJ), which uses only two transpancreatic sutures with buttresses (PJt), and compared the surgical outcomes with previously used methods, especially for hard pancreases.
METHODS
A total of 101 patients who underwent pancreaticoduodenectomy with hard pancreases were enrolled and divided into 3 groups according to the method of pancreaticoenteric anastomosis: 30 patients (29.7%) underwent the conventional dunking method (Du), 31 patients (30.7%) underwent pancreaticogastrostomy using transpancreatic sutures (PGt) and 40 patients (39.6%) underwent PJ using transpancreatic sutures (PJt). The surgical outcomes were compared according to the type of anastomosis to analyze the feasibility and ease of each technique.
RESULTS
The overall operative time was shorter in the PJt group (325.1 +/- 63.8 minutes) than in the PGt group (367.3 +/- 70.5 minutes) or the Du group (412.0 +/- 38.2 minutes, P < 0.001). In terms of pancreaticoenteric anastomosis time, it was also shorter in the PJt group (10.3 +/- 3.5 minutes) than in the Du group (20.7 +/- 0.7 minutes) or the PGt group (16.8 +/- 5.4 minutes, P = 0.005). Significant postoperative pancreatic fistula (POPF) developed in 2 cases (6.7%) in the Du group, whereas there were no POPF cases in the PGt or PJt groups (P = 0.086). Overall postoperative morbidities occurred in 31 cases (30.7%), and there were no significant differences among the 3 groups (P = 0.692).
CONCLUSION
The novel PJ technique, which uses only two transpancreatic sutures with buttresses, is a very simple, easy and secure method for hard pancreases and can be performed in a shorter amount of time compared with conventional methods.
MeSH Terms
Figure
-
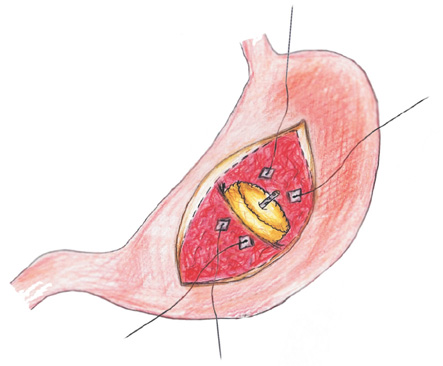
Fig. 1 A schematic diagram of pancreaticogastrostomy using two transpancreatic sutures with buttresses through a gastrostomy made in the anterior wall of stomach.

Fig. 2 The hardness of the pancreas has been estimated based on the surgeon's judgment during the operation and more objectively using a durometer to measure the hardness of the pancreas.

Fig. 3 Schematic diagrams of pancreaticogastrostomy using two transpancreatic sutures with buttresses (A) and pancreaticojejunostomy using two transpancreatic sutures with buttresses (B) after the completion of the reconstruction.

Fig. 4 Operative view (A, B) and schematic diagram (C) of pancreaticojejunostomy using two transpancreatic sutures with buttresses.
Reference
-
1. Belyaev O, Rosenkranz S, Munding J, Herzog T, Chromik AM, Tannapfel A, et al. Quantitative assessment and determinants of suture-holding capacity of human pancreas. J Surg Res. 2013; 184:807–812.2. Hong TH, Youn YC, You YK, Kim DG. An easy and secure pancreaticogastrostomy after pancreaticoduodenectomy: transpancreatic suture with a buttress method through an anterior gastrotomy. J Korean Surg Soc. 2011; 81:332–338.3. Foitzik T, Gock M, Schramm C, Prall F, Klar E. Octreotide hardens the pancreas. Langenbecks Arch Surg. 2006; 391:108–112.4. Belyaev O, Herden H, Meier JJ, Muller CA, Seelig MH, Herzog T, et al. Assessment of pancreatic hardness-surgeon versus durometer. J Surg Res. 2010; 158:53–60.5. Batignani G, Fratini G, Zuckermann M, Bianchini E, Tonelli F. Comparison of Wirsung-jejunal duct-to-mucosa and dunking technique for pancreatojejunostomy after pancreatoduodenectomy. Hepatobiliary Pancreat Dis Int. 2005; 4:450–455.6. Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery. 2005; 138:8–13.7. Walters DM, Stokes JB, Adams RB, Bauer TW. Use of a falciform ligament pedicle flap to decrease pancreatic fistula after distal pancreatectomy. Pancreas. 2011; 40:595–599.8. Kim WS, Choi DW, Choi SH, Heo JS, Kim MJ, Song SC, et al. Clinical validation of the ISGPF classification and the risk factors of pancreatic fistula formation following duct-to-mucosa pancreaticojejunostomy by one surgeon at a single center. J Gastrointest Surg. 2011; 15:2187–2192.9. Kuramoto M, Ikeshima S, Shimada S, Yamamoto K, Masuda T, Nakamura K, et al. Pancreaticojejunostomy by reinforcing the pancreas without covering the anastomotic line reduces pancreatic fistula. Int J Surg. 2013; 11:909–913.10. Wente MN, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, Izbicki JR, et al. Delayed gastric emptying (DGE) after pancreatic surgery: a suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery. 2007; 142:761–768.11. Wente MN, Veit JA, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, et al. Postpancreatectomy hemorrhage (PPH): an International Study Group of Pancreatic Surgery (ISGPS) definition. Surgery. 2007; 142:20–25.12. Topal B, Fieuws S, Aerts R, Weerts J, Feryn T, Roeyen G, et al. Pancreaticojejunostomy versus pancreaticogastrostomy reconstruction after pancreaticoduodenectomy for pancreatic or periampullary tumours: a multicentre randomised trial. Lancet Oncol. 2013; 14:655–662.13. Figueras J, Sabater L, Planellas P, Munoz-Forner E, Lopez-Ben S, Falgueras L, et al. Randomized clinical trial of pancreaticogastrostomy versus pancreaticojejunostomy on the rate and severity of pancreatic fistula after pancreaticoduodenectomy. Br J Surg. 2013; 100:1597–1605.14. Rault A, SaCunha A, Klopfenstein D, Larroude D, Epoy FN, Collet D, et al. Pancreaticojejunal anastomosis is preferable to pancreaticogastrostomy after pancreaticoduodenectomy for longterm outcomes of pancreatic exocrine function. J Am Coll Surg. 2005; 201:239–244.15. Lemaire E, O'Toole D, Sauvanet A, Hammel P, Belghiti J, Ruszniewski P. Functional and morphological changes in the pancreatic remnant following pancreaticoduodenectomy with pancreaticogastric anastomosis. Br J Surg. 2000; 87:434–438.16. Ohigashi H, Ishikawa O, Eguchi H, Sasaki Y, Yamada T, Kishi K, et al. A simple and safe anastomosis in pancreaticogastrostomy using mattress sutures. Am J Surg. 2008; 196:130–134.17. Neychev VK, Saldinger PF. Minimizing shear and compressive stress during pancreaticojejunostomy: rationale of a new technical modification. JAMA Surg. 2014; 149:203–207.18. Torer N, Ezer A, Nursal TZ. Mattress sutures for the modification of end-to-end dunking pancreaticojejunostomy. Hepatobiliary Pancreat Dis Int. 2013; 12:556–558.19. Peng SY, Wang JW, Lau WY, Cai XJ, Mou YP, Liu YB, et al. Conventional versus binding pancreaticojejunostomy after pancreaticoduodenectomy: a prospective randomized trial. Ann Surg. 2007; 245:692–698.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A novel pancreaticogastrostomy method using only two transpancreatic sutures: early postoperative surgical results compared with conventional pancreaticojejunostomy
- An easy and secure pancreaticogastrostomy after pancreaticoduodenectomy: transpancreatic suture with a buttress method through an anterior gastrotomy
- Modified Dunking Pancreaticojejunostomy
- Binding Pancreaticojejunostomy Compared with Dunking Pancreaticojejunostomy
- Pancreaticogastrostomy as a Beneficial Alternative to a Pancreaticojejunostomy
