Randomized Controlled Trial for Efficacy of Capsular Distension for Adhesive Capsulitis: Fluoroscopy-Guided Anterior Versus Ultrasonography-Guided Posterolateral Approach
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea. jijibaeheiwon@hanmail.net
- 2Department of Pathology, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea.
- KMID: 2165754
- DOI: http://doi.org/10.5535/arm.2014.38.3.360
Abstract
OBJECTIVE
To find the most effective procedure to treat adhesive capsulitis of the shoulder, we evaluated the clinical effects of an ultrasonographic-guided anterior approach capsular distension and a fluoroscopy-guided posterolateral approach capsular distension. We expected the anterior approach to be better than the posterolateral approach because the rotator interval, a triangular anatomic area in the anterosuperior aspect of the shoulder, which is considered an important component of the pathology of adhesive capsulitis.
METHODS
Participants were randomly assigned to two groups: 27 patients in group A were injected by an anterior approach with 2% lidocaine (5 mL), contrast dye (5 mL), triamcinolone (40 mg), and normal saline (9 mL) under fluoroscopic guidance in the operating room. Twenty-seven patients in group B were injected using a posterolateral approach with 2% lidocaine (5 mL), triamcinolone (40 mg), and normal saline (14 mL) under ultrasonographic guidance. After injection, all patients received physiotherapy four times in the first postoperative week and then two times each week for eight more weeks. Treatment effects were assessed using the shoulder pain and disability index (SPADI), visual numeric scale (VNS), passive range of motion (PROM), hand power (grip and pinch) at baseline and at one week, five and nine weeks after injection.
RESULTS
SPADI, VNS, PROM, and hand power improved in one week, five and nine weeks in both groups. Statistically significant differences were not observed in SPADI, VNS, PROM, or hand power between groups.
CONCLUSION
Ultrasonography-guided capsular distension by a posterolateral approach has similar effects to fluoroscopy-guided capsular distension by an anterior approach.
Keyword
MeSH Terms
Figure
-
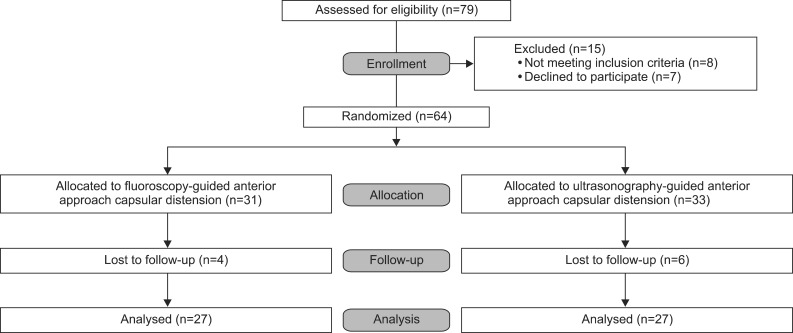
Fig. 1 Patient flowchart.
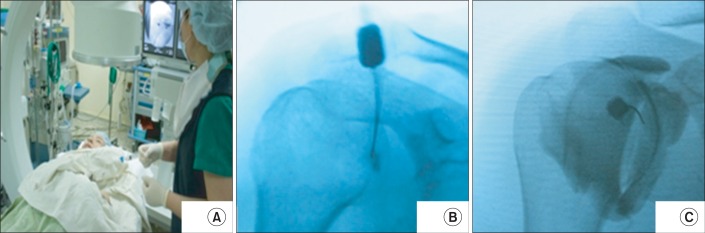
Fig. 2 Fluoroscopy-guided capsular distension method. (A) The participants were put in a supine position with a C-arm adjusted in the operating room. (B) Needle placement was confirmed in a glenohumeral arthrogram after injection of 1 mL of nonionic radiopaque contrast material. (C) After confirmation, 2% lidocaine (5 mL), contrast dye (5 mL), triamcinolone (40 mg), and normal saline (9 mL), for a total volume of 20 mL, were injected under fluoroscopic imaging.

Fig. 3 Ultrasonography-guided capsular distension method. (A) The participants were put in a sitting position in a chair, and the affected shoulder was adducted and internally rotated and the elbow flexed to grasp the contralateral shoulder. (B) The joint injection was performed using a posterolateral approach with a 23-gauge needle under sono-guidance. (C) After needle placement confirmation, 2% lidocaine (5 mL), triamcinolone (40 mg), and normal saline (14 mL), for a total volume of 20 mL fluid, were injected under sono-guidance.
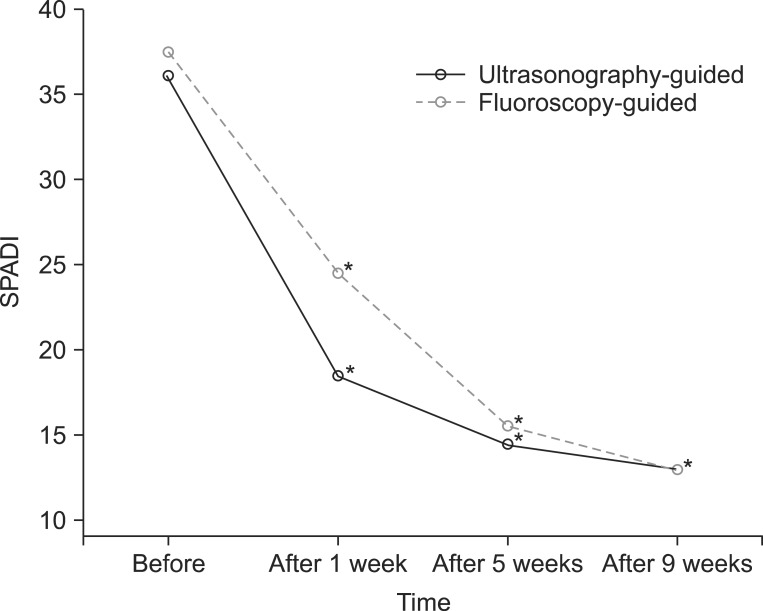
Fig. 4 Comparison of shoulder pain and disability index (SPADI) after capsular distension. SPADI was significantly improved in both groups (*p<0.05). However, no statistically significant difference in the changes of SPADI was found between the two groups.
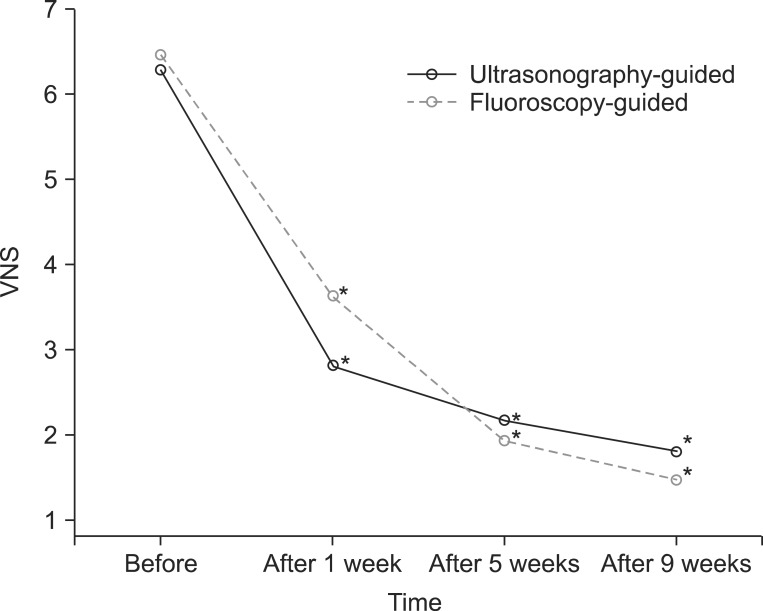
Fig. 5 Comparison of visual numeric scale (VNS) after capsular distension. VNS was significantly improved in groups A and B (*p<0.05). However, no statistically significant difference in the VNS changes was found between the two groups.
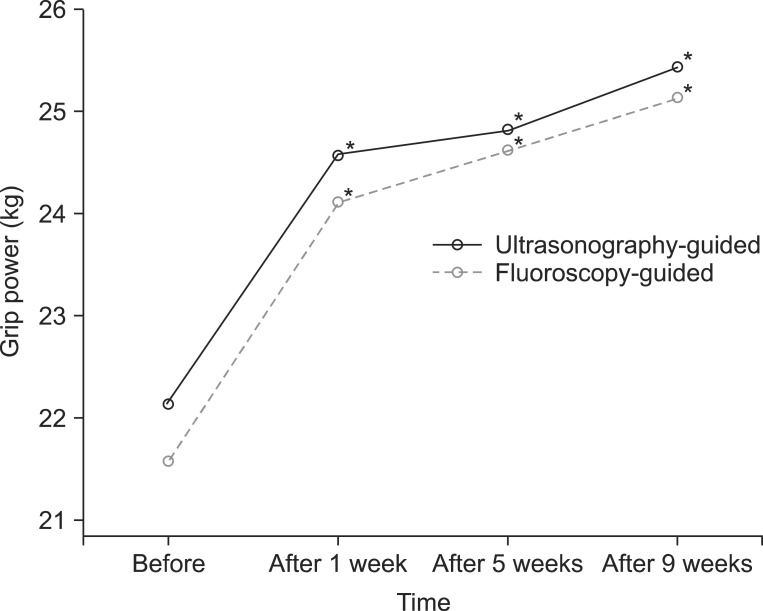
Fig. 6 Comparison of grip power after capsular distension. Grip power (kg) was significantly improved in the two groups (*p<0.05). However, no statistically significant difference in the changes of grip power was found between the two groups.
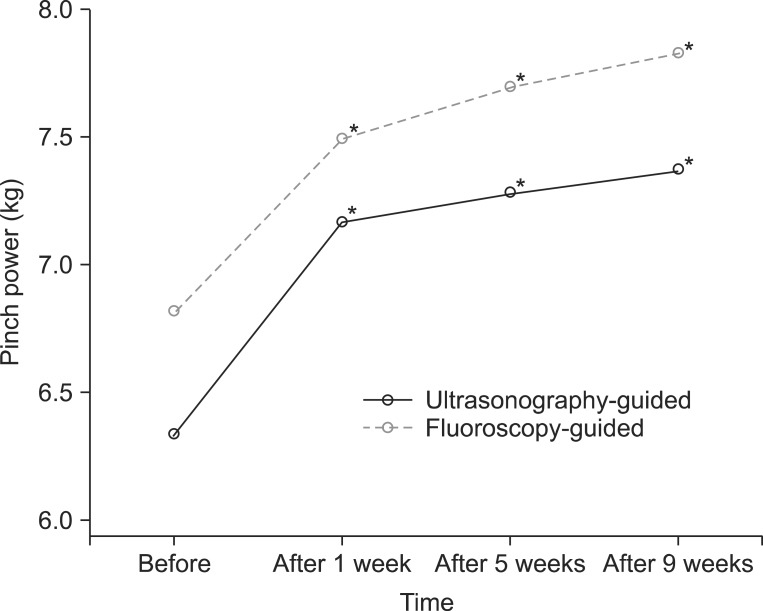
Fig. 7 Comparison of pinch power after capsular distension. Pinch power (kg) was significantly improved in the two groups (*p<0.05). However, no statistically significant difference in changes of pinch power was found between the two groups.
Reference
-
1. Neviaser AS, Neviaser RJ. Adhesive capsulitis of the shoulder. J Am Acad Orthop Surg. 2011; 19:536–542. PMID: 21885699.
Article2. Rizk TE, Pinals RS. Frozen shoulder. Semin Arthritis Rheum. 1982; 11:440–452. PMID: 7048533.
Article3. Marx RG, Malizia RW, Kenter K, Wickiewicz TL, Hannafin JA. Intra-articular corticosteroid injection for the treatment of idiopathic adhesive capsulitis of the shoulder. HSS J. 2007; 3:202–207. PMID: 18751795.
Article4. Griesser MJ, Harris JD, Campbell JE, Jones GL. Adhesive capsulitis of the shoulder: a systematic review of the effectiveness of intra-articular corticosteroid injections. J Bone Joint Surg Am. 2011; 93:1727–1733. PMID: 21938377.5. Huang CC, Tsao SL, Cheng CY, Hsin MT, Chen CM. Treating frozen shoulder with ultrasound-guided pulsed mode radiofrequency lesioning of the suprascapular nerve: two cases. Pain Med. 2010; 11:1837–1840. PMID: 21040432.
Article6. Chen HS, Chang KH, Kang JH, Hsu YH, Hsu AC, Chen SC. Treatment of frozen shoulder with intra-articular injection of botulinum toxin in shoulder joints. Med Hypotheses. 2011; 77:305–307. PMID: 21640488.
Article7. Thomas WJ, Jenkins EF, Owen JM, Sangster MJ, Kirubanandan R, Beynon C, et al. Treatment of frozen shoulder by manipulation under anaesthetic and injection: does the timing of treatment affect the outcome? J Bone Joint Surg Br. 2011; 93:1377–1381. PMID: 21969438.8. Andren L, Lundberg BJ. treatment of rigid shoulders by joint distension during arthrography. Acta Orthop Scand. 1965; 36:45–53. PMID: 14308098.9. Quraishi NA, Johnston P, Bayer J, Crowe M, Chakrabarti AJ. Thawing the frozen shoulder: a randomised trial comparing manipulation under anaesthesia with hydrodilatation. J Bone Joint Surg Br. 2007; 89:1197–1200. PMID: 17905957.10. Piotte F, Gravel D, Moffet H, Fliszar E, Roy A, Nadeau S, et al. Effects of repeated distension arthrographies combined with a home exercise program among adults with idiopathic adhesive capsulitis of the shoulder. Am J Phys Med Rehabil. 2004; 83:537–546. PMID: 15213478.
Article11. Park KD, Nam HS, Lee JK, Kim YJ, Park Y. Treatment effects of ultrasound-guided capsular distension with hyaluronic acid in adhesive capsulitis of the shoulder. Arch Phys Med Rehabil. 2013; 94:264–270. PMID: 23063625.
Article12. Vad VB, Sakalkale D, Warren RF. The role of capsular distention in adhesive capsulitis. Arch Phys Med Rehabil. 2003; 84:1290–1292. PMID: 13680563.13. Tveita EK, Tariq R, Sesseng S, Juel NG, Bautz-Holter E. Hydrodilatation, corticosteroids and adhesive capsulitis: a randomized controlled trial. BMC Musculoskelet Disord. 2008; 9:53. PMID: 18423042.
Article14. Gondim Teixeira PA, Balaj C, Chanson A, Lecocq S, Louis M, Blum A. Adhesive capsulitis of the shoulder: value of inferior glenohumeral ligament signal changes on T2-weighted fat-saturated images. AJR Am J Roentgenol. 2012; 198:W589–W596. PMID: 22623575.15. Gaskill TR, Braun S, Millett PJ. The rotator interval: pathology and management. Arthroscopy. 2011; 27:556–567. PMID: 21295939.
Article16. Harryman DT 2nd, Sidles JA, Harris SL, Matsen FA 3rd. The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am. 1992; 74:53–66. PMID: 1734014.
Article17. Ewald A. Adhesive capsulitis: a review. Am Fam Physician. 2011; 83:417–422. PMID: 21322517.18. Park KD, Nam HS, Kim TK, Kang SH, Lim MH, Park Y. Comparison of sono-guided capsular distension with fluoroscopically capsular distension in adhesive capsulitis of shoulder. Ann Rehabil Med. 2012; 36:88–97. PMID: 22506240.
Article19. Uhthoff HK, Boileau P. Primary frozen shoulder: global capsular stiffness versus localized contracture. Clin Orthop Relat Res. 2007; 456:79–84. PMID: 17179778.20. Park SK, Nam MH, Yune SH. Hydraulic management of frozen shoulder. J Korean Acad Rehabil Med. 1992; 16:147–153.21. Levine WN, Kashyap CP, Bak SF, Ahmad CS, Blaine TA, Bigliani LU. Nonoperative management of idiopathic adhesive capsulitis. J Shoulder Elbow Surg. 2007; 16:569–573. PMID: 17531513.
Article22. Park GY, Hwang SE. Comparison of intraarticular steroid injection with and without capsular distension in adhesive capsulitis of the shoulder. J Korean Acad Rehabil Med. 2000; 24:1174–1179.23. Choi ES, Kim JS, Lee YS, Shin BS, Ko YJ, Park SH. Arthrographic findings of frozen shoulder and therapeutic effect of distension arthrography. J Korean Acad Rehabil Med. 2001; 25:278–283.24. Kim JS, Kwon JY, Lee WI, Kim JM. The additional effect of tear after passive exercise during distension arthrography in patients with frozen shoulder. J Korean Acad Rehabil Med. 2008; 32:324–326.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Sono-guided Capsular Distension with Fluoroscopically Capsular Distension in Adhesive Capsulitis of Shoulder
- Comparison of Intraarticular Steroid Injection with and without Capsular Distension in Adhesive Capsulitis of the Shoulder
- Updates on the treatment of adhesive capsulitis with hydraulic distension
- The Success Rate of Posterior Approach Glenohumeral Injection in Patients with Adhesive Capsulitis
- Adhesive Capsulitis of the Shoulder
