Solitary Primary Leptomeningeal Glioma: Case Report
- Affiliations
-
- 1Department of Neurosurgery, Yonsei University College of Medicine, Seoul, Korea. changjh@yuhs.ac
- 2Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- 3Neuro-Oncology Clinic, Yonsei University College of Medicine, Seoul, Korea.
- 4Brain Research Institute, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2165221
- DOI: http://doi.org/10.14791/btrt.2013.1.1.36
Abstract
- We report a case of solitary primary leptomeningeal glioma. The mass was totally removed under awake surgery. Intraoperatively, no parenchymal involvement was noted. Histopathological study revealed a predominant anaplastic oligodendroglioma component and a focal anaplastic astrocytoma component, which was consistent with an anaplastic oligoastrocytoma. Adjuvant tomotherapy was followed and the tumor has not recurred until 12 months after surgery. A focal type of primary leptomeningeal glioma is extremely rare. We report a rare case of solitary primary leptomeningeal anaplastic oligoastrocytoma.
Keyword
MeSH Terms
Figure
-

Fig. 1 Preoperative computed tomography shows a suspicious tumor mass on the right medial frontal lobe (A). Magnetic resonance imaging (MRI) revealed heterogeneous subtle enhancement on T1-weighted images (B and C). T2-weighted MRI showed well-circumscribed tumor mass with superficial siderosis (arrowheads) (D).
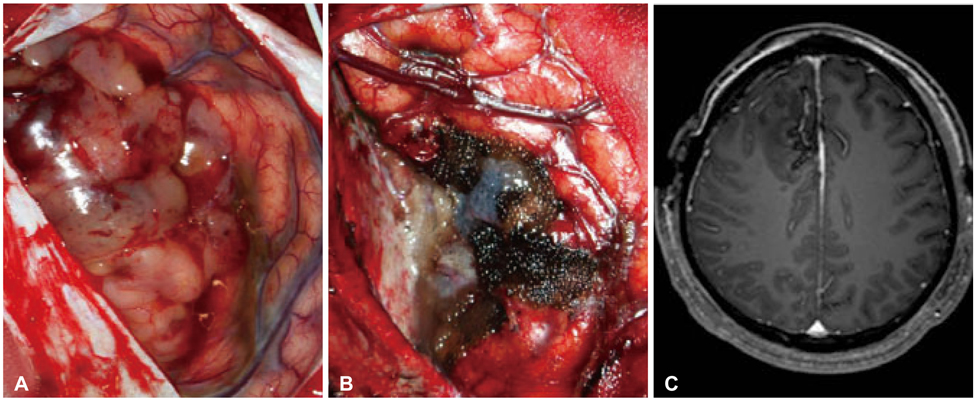
Fig. 2 The tumor is grayish and distinguished from normal brain by gross appearance (A). There was no continuation between tumor mass and surrounding normal brain. The tumor was totally removed (B), which was confirmed on immediate postoperative magnetic resonance imaging (C).

Fig. 3 Low power view shows relatively well-circumscribed tumor mass (A). High power view demonstrates glial tumor cells with increased cellularity (B). The majority of tumor cells are small round cells with a perinuclear halo, which is consistent with anaplastic oligodendroglioma (C). However, astrocytic tumor component was also observed in a small part of the tumor (D). A: H&E 12×. B: H&E 100×. C and D: H&E 400×.

Fig. 4 By immunohistochemistry (IHC) stains, the tumor cells were strong positive for glial fibrillary acidic protein (GFAP) and Olig-2 (A, B). IHC also revealed that isocitrate dehydrogenase 1 (IDH1) was mutated (C) and epidermal growth factor receptor (EGFR) was amplified (D). Ki-67 proliferative index was about 10-15% (E). A: GFAP-IHC 200×. B: Olig-2-IHC 200×. C: IDH1-IHC 200×. D: EGFR-IHC 200×. E: Ki-67-IHC 200×.
Cited by 1 articles
-
Primary Diffuse Leptomeningeal Gliosarcomatosis
Ju Hyung Moon, Se Hoon Kim, Eui Hyun Kim, Seok-Gu Kang, Jong Hee Chang
Brain Tumor Res Treat. 2015;3(1):34-38. doi: 10.14791/btrt.2015.3.1.34.
Reference
-
1. Kakita A, Wakabayashi K, Takahashi H, Ohama E, Ikuta F, Tokiguchi S. Primary leptomeningeal glioma: ultrastructural and laminin immunohistochemical studies. Acta Neuropathol. 1992; 83:538–542.
Article2. Kalyan-Raman UP, Cancilla PA, Case MJ. Solitary, primary malignant astrocytoma of the spinal leptomeninges. J Neuropathol Exp Neurol. 1983; 42:517–521.
Article3. Opeskin K, Anderson RM, Nye DH. Primary meningeal glioma. Pathology. 1994; 26:72–74.
Article4. De Tommasi A, Occhiogrosso G, De Tommasi C, Luzzi S, Cimmino A, Ciappetta P. A polycystic variant of a primary intracranial leptomeningeal astrocytoma: case report and literature review. World J Surg Oncol. 2007; 5:72.
Article5. Cooper IS, Kernohan JW. Heterotopic glial nests in the subarachnoid space; histopathologic characteristics, mode of origin and relation to meningeal gliomas. J Neuropathol Exp Neurol. 1951; 10:16–29.
Article6. Keith T, Llewellyn R, Harvie M, Roncaroli F, Weatherall MW. A report of the natural history of leptomeningeal gliomatosis. J Clin Neurosci. 2011; 18:582–585.
Article7. Horoupian DS, Lax F, Suzuki K. Extracerebral leptomeningeal astrocytoma mimicking a meningioma. Arch Pathol Lab Med. 1979; 103:676–679.8. Thomas JE, Falls E, Velasco ME, Zaher A. Diagnostic value of immunocytochemistry in leptomeningeal tumor dissemination. Arch Pathol Lab Med. 2000; 124:759–761.
Article9. Bailey P, Robitaille Y. Primary diffuse leptomeningeal gliomatosis. Can J Neurol Sci. 1985; 12:278–281.
Article10. Scully RE, Galdabini JJ, McNeely BU. Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 17-1978. N Engl J Med. 1978; 298:1014–1021.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Primary Diffuse Leptomeningeal Gliomatosis: Report of a Case Presenting with Chronic Meningitis
- Response of Leptomeningeal Dissemination of Anaplastic Glioma to Temozolomide: Experience of Two Cases
- The Clinical Features of Spinal Leptomeningeal Dissemination from Malignant Gliomas
- Primary Diffuse Leptomeningeal Gliosarcomatosis
- Leptomeningeal Dissemination of a Low-Grade Brainstem Glioma without Local Recurrence
