Two Cases of Cerebral Air Embolism That Occurred during Esophageal Ballooning and Endoscopic Retrograde Cholangiopancreatography
- Affiliations
-
- 1Department of Gastroenterology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. ji110@hanmail.net
- 2Department of Neurology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2165045
- DOI: http://doi.org/10.5946/ce.2015.071
Abstract
- Cerebral air embolism is an extremely rare complication of endoscopic procedure and often life threatening. We present two cases of cerebral infarction due to air embolization caused by an endoscopic intervention. The first case occurred during esophageal balloon dilatation for the treatment of a stricture of an anastomosis site in a 59-year-old man and the second case occurred during endoscopic papillary balloon dilatation in a 69-year-old man who had distal common bile duct stones. After the procedure, cardiopulmonary instability and altered mental status were observed in both patients, and cerebral air embolism was diagnosed in both cases. Hyperbaric oxygen therapy was started in the first case, and high FiO2 therapy was applied in the second case. Although this complication is rare, patient outcomes can be improved if physicians are aware of this potential complication, and immediately begin proper management.
Keyword
MeSH Terms
Figure
-
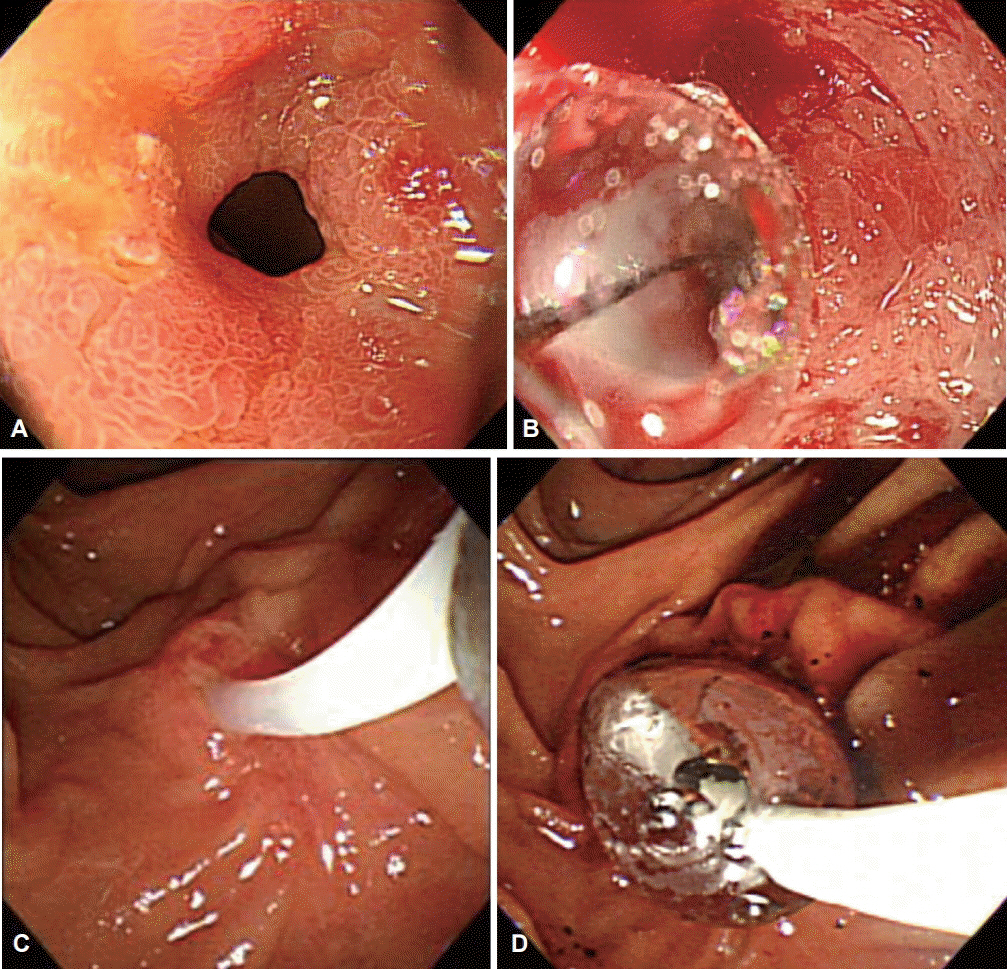
Fig. 1. Endoscopic procedures for the study patients. (A, B) Through-the-scope balloon dilatation was performed in case 1, and (C, D) endoscopic retrograde papillary drainage in case 2. (A) An initial esophagogastroduodenoscopy showed an esophageal stricture at the esophagojejunostomy anastomotic ring. (B) Through-the-scope balloon dilatation was performed. (C) Endoscopic biliary cannulation was carried out through the major papilla. (D) Endoscopic retrograde papillary drainage with ballooning was performed.
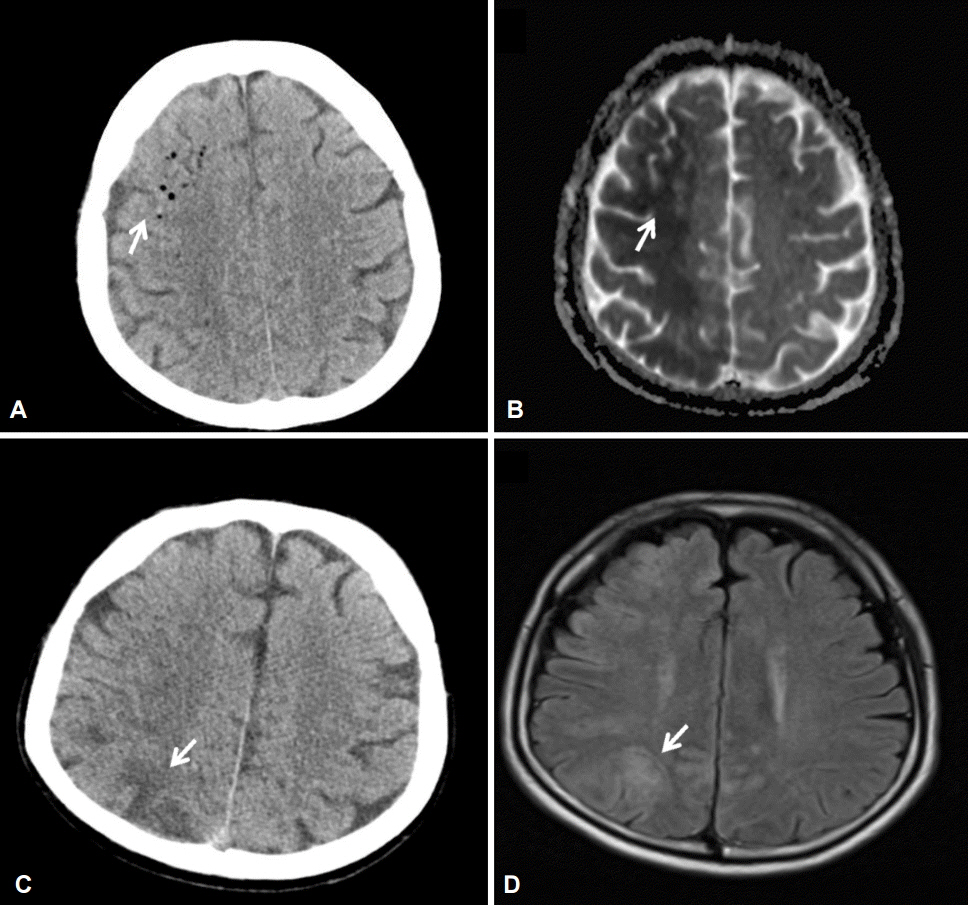
Fig. 2. Imaging studies with computed tomography (CT) and magnetic resonance imaging (MRI). (A) CT scan showing hypodense lesions indicative of air bubbles that were seen predominantly in the right hemisphere in case 1 (arrow). (B) Diffusion-weighted imaging showing diffusion restriction in the right hemisphere in case 1 (arrow). (C) MRI scan showing multiple wedge-shaped low-density regions in the right hemisphere in case 2 (arrow). (D) MRI scan showing multiple diffusion-restricted lesions and fluid-attenuated inversion recovery changes in case 2 (arrow).
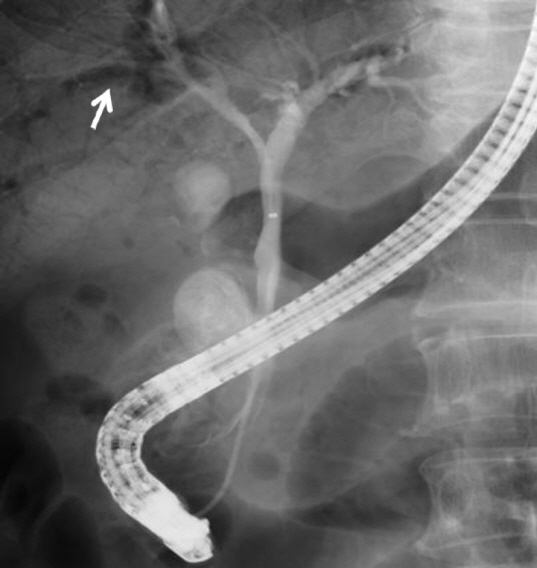
Fig. 3. Endoscopic retrograde cholangiography showing extensive air in the portal vein in case 2 (arrow).
Reference
-
1. Green J. Complications of gastrointestinal endoscopy [Internet]. London: British Society of Gastroenterology;c2009. [cited 2016 Feb 2]. Available from: http://www.bsg.org.uk/pdf_word_docs/complications.pdf.2. Silvis SE, Nebel O, Rogers G, Sugawa C, Mandelstam P. Endoscopic complications. Results of the 1974 American Society for Gastrointestinal Endoscopy Survey. JAMA. 1976; 235:928–930.3. Gangi S, Saidi F, Patel K, Johnstone B, Jaeger J, Shine D. Cardiovascular complications after GI endoscopy: occurrence and risks in a large hospital system. Gastrointest Endosc. 2004; 60:679–685.
Article4. Romagnuolo J, Cotton PB, Eisen G, Vargo J, Petersen BT. Identifying and reporting risk factors for adverse events in endoscopy. Part I: cardiopulmonary events. Gastrointest Endosc. 2011; 73:579–585.
Article5. Donepudi S, Chavalitdhamrong D, Pu L, Draganov PV. Air embolism complicating gastrointestinal endoscopy: a systematic review. World J Gastrointest Endosc. 2013; 5:359–365.
Article6. Muth CM, Shank ES. Gas embolism. N Engl J Med. 2000; 342:476–482.
Article7. Pandurangadu AV, Paul JA, Barawi M, Irvin CB. A case report of cerebral air embolism after esophagogastroduodenoscopy: diagnosis and management in the emergency department. J Emerg Med. 2012; 43:976–979.
Article8. López JC, Pérez X, Esteve F. Cerebral air embolism during upper endoscopy. Endoscopy. 2010; 42 Suppl 2:E41.
Article9. Efthymiou M, Raftopoulos S, Antonio Chirinos J, May GR. Air embolism complicated by left hemiparesis after direct cholangioscopy with an intraductal balloon anchoring system. Gastrointest Endosc. 2012; 75:221–223.
Article10. Zampeli E, Tsagalou E, Kanakakis I, et al. Fatal cerebral air embolism complicating esophageal dilation. Endoscopy. 2013; 45(Suppl 2 UCTN):E358.
Article11. Pee L, Basu S, Loganayagam A. Cerebral air embolism: a rare complication following balloon dilation. Endoscopy. 2013; 45(Suppl 2 UCTN):E93–E94.
Article12. Raju GS, Bendixen BH, Khan J, Summers RW. Cerebrovascular accident during endoscopy: consider cerebral air embolism, a rapidly reversible event with hyperbaric oxygen therapy. Gastrointest Endosc. 1998; 47:70–73.
Article13. McAree BJ, Gilliland R, Campbell DM, Lucas JW, Dickey W. Cerebral air embolism complicating esophagogastroduodenoscopy (EGD). Endoscopy. 2008; 40 Suppl 2:E191–E192.
Article14. Akhtar N, Jafri W, Mozaffar T. Cerebral artery air embolism following an esophagogastroscopy: a case report. Neurology. 2001; 56:136–137.
Article15. Weber MA, Fiebach JB, Lichy MP, Weber R, Schwark C, Grau AJ. Bilateral cerebral air embolism. J Neurol. 2003; 250:1115–1117.
Article16. Demaerel P, Gevers AM, De Bruecker Y, Sunaert S, Wilms G. Stroke caused by cerebral air embolism during endoscopy. Gastrointest Endosc. 2003; 57:134–135.
Article17. Rabe C, Balta Z, Wüllner U, et al. Biliary metal stents and air embolism: a note of caution. Endoscopy. 2006; 38:648–650.
Article18. Stabile L, Cigada M, Stillittano D, et al. Fatal cerebral air embolism after endoscopic retrograde cholangiopancreatography. Acta Anaesthesiol Scand. 2006; 50:648–649.
Article19. Goins KM, May JM, Hucklenbruch C, Littlewood KE, Groves DS. Unexpected cardiovascular collapse from massive air embolism during endoscopic retrograde cholangiopancreatography. Acta Anaesthesiol Scand. 2010; 54:385–388.
Article20. van Boxel GI, Hommers CE, Dash I, Goodman AJ, Green J, Orme RM. Myocardial and cerebral infarction due to massive air embolism following endoscopic retrograde cholangiopancreatography (ERCP). Endoscopy. 2010; 42 Suppl 2:E80–E81.
Article21. Maccarone G, Shakoor T, Ellis B. Air embolism after percutaneous transhepatic biliary drainage and subsequent endoscopic retrograde cholangiopancreatography (ERCP). Endoscopy. 2011; 43 Suppl 2 UCTN:E399.
Article22. Nern C, Bellut D, Husain N, Pangalu A, Schwarz U, Valavanis A. Fatal cerebral venous air embolism during endoscopic retrograde cholangiopancreatography: case report and review of the literature. Clin Neuroradiol. 2012; 22:371–374.23. Chavalitdhamrong D, Draganov PV. Acute stroke due to air embolism complicating ERCP. Endoscopy. 2013; 45 Suppl 2 UCTN:E177–E178.
Article24. Rangappa P, Uhde B, Byard RW, Wurm A, Thomas PD. Fatal cerebral arterial gas embolism after endoscopic retrograde cholangiopancreatography. Indian J Crit Care Med. 2009; 13:108–112.
Article25. Blanc P, Boussuges A, Henriette K, Sainty JM, Deleflie M. Iatrogenic cerebral air embolism: importance of an early hyperbaric oxygenation. Intensive Care Med. 2002; 28:559–563.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A rare but lethal complication: Post-endoscopic retrograde cholangiopancreatography cerebral arterial gas embolism
- Unusual Complications Related to Endoscopic Retrograde Cholangiopancreatography and Its Endoscopic Treatment
- Fatal Cerebral Air Embolism Due to a Patent Foramen Ovale during Endoscopic Retrograde Cholangiopancreatography
- Cerebral Air Embolism Following a Gastroscopy
- Fatal Biliary-Systemic Air Embolism during Endoscopic Retrograde Cholangiopancreatography: A Case with Multifocal Liver Abscesses and Choledochoduodenostomy
