Fatal Biliary-Systemic Air Embolism during Endoscopic Retrograde Cholangiopancreatography: A Case with Multifocal Liver Abscesses and Choledochoduodenostomy
- Affiliations
-
- 1Digestive Disease Center, CHA Bundang Medical Center, School of Medicine, CHA University, Seongnam, Korea. endoscopy@cha.ac.kr
- KMID: 1126034
- DOI: http://doi.org/10.3349/ymj.2010.51.2.287
Abstract
- We report a rare case of a massive fatal embolism that occurred in the middle of endoscopic retrograde cholangiopancreatography (ERCP) and retrospectively examine the significant causes of the event. The patient was a 50-year old female with an uncertain history of previous abdominal surgery for multiple biliary stones 20 years prior. The patient presented with acute right upper quadrant pain. An abdominal computed tomographic (CT) scan revealed the presence of multiple stones in the common bile duct (CBD) and intra-hepatic duct (IHD) with biliary obstruction, multifocal liver abscesses, and air-biliarygram. Emergency ERCP showed a wide and straight opening of choledochoduodenostomy, which may have been created during a previous surgery, and multiple filling defects in the CBD. With the use of a forward endoscope, mud stones were extracted through the opening of the choledochoduodenostomy. Cardiac arrest suddenly developed during the procedure, and despite immediate resuscitation, the patient died due to a massive systemic air embolism. We reviewed previously reported fatal cases and accessed factors facilitating air embolisms in this case.
Keyword
MeSH Terms
Figure
-

Fig. 1 Abdominal CT scan showing multiple stones in the CBD and IHD with biliary obstruction, multifocal liver abscesses, and air-biliarygram. CBD, common bile duct; IHD, intra-hepatic duct.
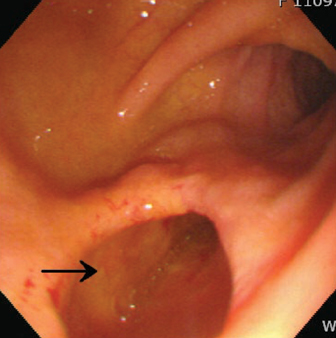
Fig. 2 ERCP showing the wide and straight opening of a choledochoduodenostomy (arrow). ERCP, endoscopic retrograde cholangiopancreatography.
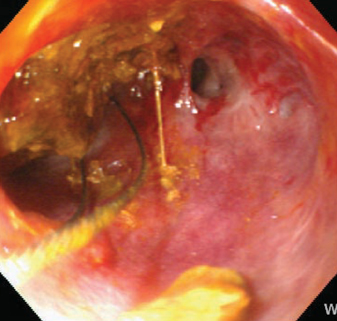
Fig. 3 Brown-pigmented mud stones (arrow) were being extracted with the forward endoscope.

Fig. 4 Chest X-ray taken at the scene revealing air density occupied in heart chambers (arrow) and hepatic vasculatures and splenic vein (arrow heads) indicating a massive air embolism.
Cited by 2 articles
-
Unusual Complications Related to Endoscopic Retrograde Cholangiopancreatography and Its Endoscopic Treatment
Chang-Il Kwon, Sang Hee Song, Ki Baik Hahm, Kwang Hyun Ko
Clin Endosc. 2013;46(3):251-259. doi: 10.5946/ce.2013.46.3.251.Fatal Cerebral Air Embolism Due to a Patent Foramen Ovale during Endoscopic Retrograde Cholangiopancreatography
Adam Bastovansky, Claudia Stöllberger, Josef Finsterer
Clin Endosc. 2014;47(3):275-280. doi: 10.5946/ce.2014.47.3.275.
Reference
-
1. Nayagam J, Ho KM, Liang J. Fatal systemic air embolism during endoscopic retrograde cholangio-pancreatography. Anaesth Intensive Care. 2004. 32:260–264.
Article2. Christi SU, Scheppach W, Peters U, Kirchner T. Cerebral air embolism after gastroduodenoscopy: complication of a duodenocaval fistula. Gastrointest Endosc. 1994. 40:376–378.3. Raju GS, Bcndixen BH, Khan J, Summers RW. Cerebrovascular accident during endoscopy: consider cerebral air embolism, a rapidly reversible event with hyperbaric oxygen therapy. Gastrointest Endosc. 1998. 47:70–73.
Article4. Akhtar N, Jafri W, Mozaffar T. Cerebral artery air embolism following an esophagogastroscopy: a case report. Neurology. 2001. 56:136–137.
Article5. Kennedy C, Larvin M, Linsell J. Fatal hepatic air embolism following ERCR. Gastrointest Endosc. 1997. 45:187–188.6. Mohammedi I, Ber C, Peguet O, Ould-Aoudia T, Duperret S, Petit P. Cardiac air embolism after endoscopic retrograde cholangiopancreatography in a patient with blunt hepatic trauma. J Trauma. 2002. 53:1170–1172.
Article7. Siddiqui J, Jaffe PE, Aziz K, Forouhar F, Sheppared R, Covault J, et al. Fatal air and bile embolism after percutaneous liver biopsy and ERCP. Gastrointest Endosc. 2005. 61:153–157.
Article8. Stabile L, Cigada M, Stillittano D, Morandi E, Zaffaroni M, Rossi G, et al. Fatal cerebral air embolism after endoscopic retrograde cholangiopancreatography. Acta Anaesthesiol Scand. 2006. 50:648–649.
Article9. Liebman PR, Patten MT, Manny J, Benfield JR, Hechtman HB. Hepatic--portal venous gas in adults: etiology, pathophysiology and clinical significance. Ann Surg. 1978. 187:281–287.10. Simmons TC. Hepatic portal venous gas due to endoscopic sphincterotomy. Am J Gastroenterol. 1988. 83:326–328.11. Barthet M, Membrini P, Bernard JP, Sahel J. Hepatic portal venous gas after endoscopic biliary sphincterotomy. Gastrointest Endosc. 1994. 40:261–263.
Article12. Herman JB, Levine MS, Long WB. Portal venous gas as a complication of ERCP and endoscopic sphincterotomy. Am J Gastroenterol. 1995. 90:828–829.13. Katzgraber F, Glenewinkel F, Rittner C, Beule J. Fatal air embolism resulting from gastroscopy. Lancet. 1995. 346:1714–1715.14. Huycke A, Moeller DD. Hepatic portal venous gas after colonoscopy in granulomatous colitis. Am J Gastroenterol. 1985. 80:637–638.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A rare but lethal complication: Post-endoscopic retrograde cholangiopancreatography cerebral arterial gas embolism
- Fatal Cerebral Air Embolism Due to a Patent Foramen Ovale during Endoscopic Retrograde Cholangiopancreatography
- Advances in Endoscopic Ultrasound-Guided Biliary Drainage: A Comprehensive Review
- Endoscopic ultrasound-guided biliary drainage in malignant distal biliary obstruction
- Unusual Complications Related to Endoscopic Retrograde Cholangiopancreatography and Its Endoscopic Treatment
