Exuberant Vasculoconnective Component in Mediastinal Mixed Germ Cell Tumors
- Affiliations
-
- 1Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. hanjho@skku.edu
- 2Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Thoracic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2164503
- DOI: http://doi.org/10.3346/jkms.2015.30.8.1085
Abstract
- We aimed to evaluate the histologic components of primary mediastinal mixed germ cell tumors. A total of 221 patients diagnosed with a mediastinal germ cell tumor (GCT) were retrospectively reviewed. Among them, 14 patients underwent surgical resection after chemotherapy and 8 patients were diagnosed with mixed GCT, who were then selected for further evaluation. Clinical chart review and histologic review of biopsy and surgical specimens of 8 patients were performed. All 8 patients were young males and showed a mature teratoma or a mature teratoma with a focal immature teratoma in the resected specimens. Serum alpha-feto protein was variably elevated. Seven patients experienced an increase in tumor size after the chemotherapy. In 5 patients, a variable amount of vasculoconnective tissue was found along with the mature teratoma occupying average 66.3% of resected mass, and 3 of them showed an identical vasculoconnective component on biopsy before chemotherapy. We suggest that vasculoconnective tissue might be the intrinsic component of primary mediastinal mixed GCT. When vasculoconnective tissue is obtained on small biopsy of an anterior mediastinal mass of a young male, the possibility of underlying mixed GCT should be considered and further clinical work up should be performed.
Keyword
MeSH Terms
Figure
-
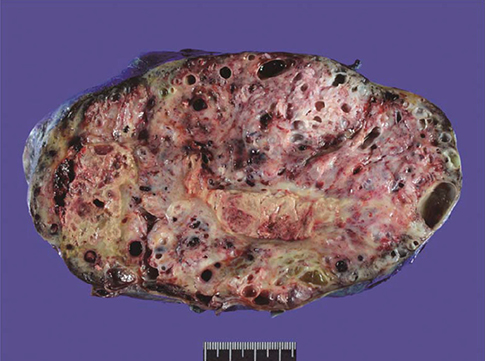
Fig. 1 Resected mediastinal mixed germ cell tumor gross specimen. The mass is well circumscribed, which corresponds to the gross feature of a teratoma. The cut surface shows necrosis, hemorrhage and cystic change.

Fig. 2 Low-power view of 5 resected mediastinal germ cell tumors after chemotherapy harboring a vasculoconnective component (Hematoxylin and eosin staining, magnification, × 12.5). With variable degrees of hemorrhage, cystically delated glandular components and cartilaginous components of the mature teratoma are easily seen. Since the vasculoconnective components are intermingled with the underlying teratoma, there is no discernable mass-like lesion under low-power magnification. (A, case 1; B, case 2; C, case 3; D, case 4; E, case 5).
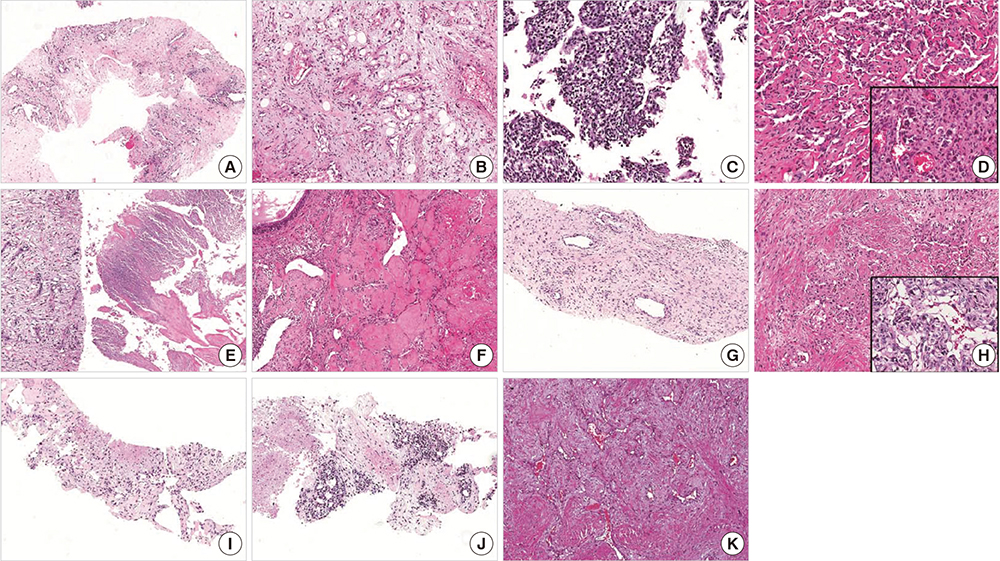
Fig. 3 Biopsy specimen before chemotherapy (A, C, E, G, I, J) and the vasculoconnective component in the resected specimen after chemotherapy (B, D, F, H, K) (Hematoxylin and eosin staining, magnification, ×40, magnification of inbox, ×200). Only two biopsy specimens (case 2, C and case 5, J) were diagnostic for a germ cell tumor (GCT). In two patients (case 2 and case 4), a variable degree of cellular atypia is found in the resected specimen (D and H, inbox). In case 5, the first biopsy shows no identifiable GCT component (I). However, in the second biopsy, an embryonal carcinoma-like area is detected (J). Histological features of the vasculoconnective components were insufficient for diagnosis of angiosarcoma (Case 1, A and B; Case 2, C and D; Case 3, E and F; Case 4, G and H; Case 5, I, J, and K).
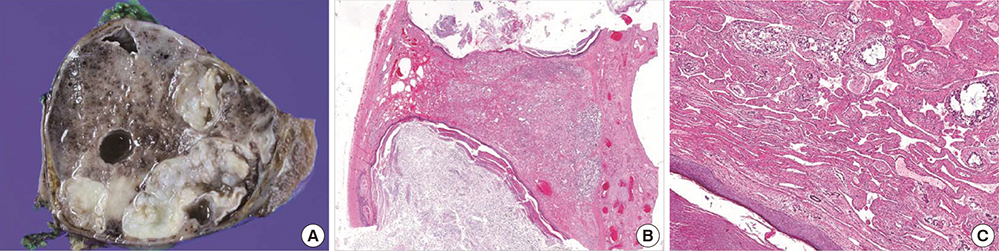
Fig. 4 A resected mediastinal mass without prior chemotherapy from an 18-yr-old male patient. Grossly, the mass is well circumscribed, and hemorrhage and cystic changes are found on the cut surface (A). Microscopically, the mass is composed of a mature teratoma, yolk sac tumor, and an abundant vasculoconnective component (B, Hematoxylin and eosin staining, magnification, ×12.5). On high-power view, the vasculoconnective component is seen to be intermingled with the yolk sac tumor (C, Hematoxylin and eosin staining, magnification, ×100). An epidermal element with keratin is seen in the left lower corner (C).
Reference
-
1. Rusner C, Trabert B, Katalinic A, Kieschke J, Emrich K, Stang A. Network of German Cancer Registries (GEKID). Incidence patterns and trends of malignant gonadal and extragonadal germ cell tumors in Germany, 1998-2008. Cancer Epidemiol. 2013; 37:370–373.2. Stang A, Trabert B, Wentzensen N, Cook MB, Rusner C, Oosterhuis JW, McGlynn KA. Gonadal and extragonadal germ cell tumours in the United States, 1973-2007. Int J Androl. 2012; 35:616–625.3. Albany C, Einhorn LH. Extragonadal germ cell tumors: clinical presentation and management. Curr Opin Oncol. 2013; 25:261–265.4. Takeda S, Miyoshi S, Akashi A, Ohta M, Minami M, Okumura M, Masaoka A, Matsuda H. Clinical spectrum of primary mediastinal tumors: a comparison of adult and pediatric populations at a single Japanese institution. J Surg Oncol. 2003; 83:24–30.5. Moran CA, Suster S. Primary germ cell tumors of the mediastinum: I. Analysis of 322 cases with special emphasis on teratomatous lesions and a proposal for histopathologic classification and clinical staging. Cancer. 1997; 80:681–690.6. Weidner N. Germ-cell tumors of the mediastinum. Semin Diagn Pathol. 1999; 16:42–50.7. Malagón HD, Valdez AM, Moran CA, Suster S. Germ cell tumors with sarcomatous components: a clinicopathologic and immunohistochemical study of 46 cases. Am J Surg Pathol. 2007; 31:1356–1362.8. Akbulut M, Zekioglu O, Terek MC, Ozdemir N. Florid vascular proliferation in mature cystic teratoma of the ovary: case report and review of the literature. Tumori. 2009; 95:104–107.9. Itoh H, Wada T, Michikata K, Sato Y, Seguchi T, Akiyama Y, Kataoka H. Ovarian teratoma showing a predominant hemangiomatous element with stromal luteinization: report of a case and review of the literature. Pathol Int. 2004; 54:279–283.10. Baker PM, Rosai J, Young RH. Ovarian teratomas with florid benign vascular proliferation: a distinctive finding associated with the neural component of teratomas that may be confused with a vascular neoplasm. Int J Gynecol Pathol. 2002; 21:16–21.11. Gaudin PB, Rosai J. Florid vascular proliferation associated with neural and neuroendocrine neoplasms. A diagnostic clue and potential pitfall. Am J Surg Pathol. 1995; 19:642–652.12. Logothetis CJ, Samuels ML, Trindade A, Johnson DE. The growing teratoma syndrome. Cancer. 1982; 50:1629–1635.13. D'Aiuto M, Veronesi G, Peccatori FA, Pelosi G, Venturino M, Gasparri R, Presicci F, Galetta D, Spaggiari L. Mediastinal-like growing teratoma syndrome. J Thorac Cardiovasc Surg. 2005; 130:228–229.14. André F, Fizazi K, Culine S, Droz J, Taupin P, Lhommé C, Terrier-Lacombe M, Théodore C. The growing teratoma syndrome: results of therapy and long-term follow-up of 33 patients. Eur J Cancer. 2000; 36:1389–1394.15. Afifi HY, Bosl GJ, Burt ME. Mediastinal growing teratoma syndrome. Ann Thorac Surg. 1997; 64:359–362.16. Agatsuma T, Koizumi T, Kubo K, Saito G, Kondo R, Yoshida K, Ito K, Endo M, Shimojo H. Mediastinal growing teratoma syndrome successfully treated by multiple modality therapies. Intern Med. 2011; 50:607–610.17. Chen LT, Chen CL, Hwang WS. The growing teratoma syndrome. A case of primary mediastinal nonseminomatous germ cell tumor treated with chemotherapy and radiotherapy. Chest. 1990; 98:231–233.18. Hayashi M, Igarashi N, Fujimori F, Kuriyama H, Ebe Y, Nishibori T, Sato K, Hosaka Y, Yamato Y, Togashi K, et al. A case of mediastinal growing teratoma syndrome with acute megakaryoblastic leukemia. Gan To Kagaku Ryoho. 2014; 41:869–873.19. Hirai Y, Yoshimasu T, Oura S, Okamura Y. Mediastinal germ cell tumor with acute myeloid leukemia and growing teratoma syndrome. Interact Cardiovasc Thorac Surg. 2011; 12:96–97.20. Iyoda A, Hiroshima K, Yusa T, Toyozaki T, Fujisawa T, Ohwada H. The primary mediastinal growing teratoma syndrome. Anticancer Res. 2000; 20:3723–3726.21. Kesler KA, Patel JB, Kruter LE, Birdas TJ, Rieger KM, Okereke IC, Einhorn LH. The "growing teratoma syndrome" in primary mediastinal nonseminomatous germ cell tumors: criteria based on current practice. J Thorac Cardiovasc Surg. 2012; 144:438–443.22. Massard G, Eichler F, Gasser B, Bergerat JP, Wihlm JM. Recurrence of the mediastinal growing teratoma syndrome. Ann Thorac Surg. 1998; 66:605–606.23. Nuti R, Bodhireddy S, Thirumala S. Mixed germ cell tumor of mediastinum/lung masquerading as hemangioma in fine needle biopsy. Indian J Pathol Microbiol. 2013; 56:158–160.24. Hui M, Tandon A, Uppin SG, Paruchuri RK. Postchemotherapy-related changes in mediastinal mixed germ cell tumor masquerading as a vascular neoplasm. Indian J Pathol Microbiol. 2012; 55:531–534.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Mixed Germ Cell Tumor with 6 Components of Germ Cell and Sarcomatous Component
- Computed tomographic findings of malignant ovarian germ cell tumors
- A Case of Mixed Germ Cell Tumor of the Mediastinum
- A Case of Combined Mixed Germ Cell Tumor and Angiosarcoma within the Mediastinum
- Suprasellar Mixed Germ Cell Tumor: Case Report
