Tailgut cyst accompanied with bony defect
- Affiliations
-
- 1Department of Neurosurgery, Soonchunhyang University Cheonan Hospital, Cheonan, Korea. metatron1324@naver.com
- KMID: 2160955
- DOI: http://doi.org/10.4174/astr.2016.90.4.235
Abstract
- Retro-rectal cystic hamartoma (tailgut cyst), is an uncommon congenital developmental lesion, generally located in the retro-rectal space. Its diagnosis and approach is challenging because the retropelvic space is not familiar. We report a 51-year-old woman who presented with paresthesia and pain in perianal area. The magnetic resonance image showed high signal intensity on the T1-weighted image and iso to high signal intensity on the T2-weighted image of the retropelvic space and CT showed sacral bony defect. We chose the posterior approach for removal of the tailgut cyst. Histopathology exam of the retropelvic cyst revealed a multiloculated cyst containing abundant mucoid material lined by both squamous and glandular mucinous epithelium. The patient has recovered nicely with no recurrence. Tailgut cyst needs complete surgical excision for good prognosis. So, a preoperative high-resolution image and co-operation between neurosurgen and general surgeon would help to make safe and feasible diagnosis and surgical access.
MeSH Terms
Figure
-

Fig. 1 Pelvic CT showing bony defect on lower sacral bone (about S3–S4) near cyst (white arrow).
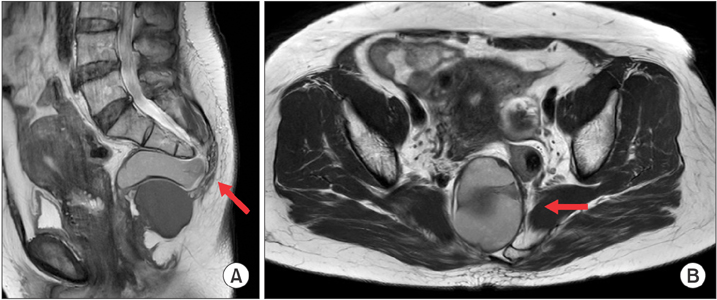
Fig. 2 Pelvic MRI with gadolinium enhancement showing Iso to high signal intensity on T2-weighted image (A: sagittal, B: axial). Size of mass was about 6 cm, of which the multilobulated mass was on sacrococcygeal area (red arrow). Uterus was enlarged and heterogeneously enhanced.

Fig. 3 (A) After sacral laminectomy, cyst demonstrating well-marginated and capsulated, connected with some dural ends. Small incision was made on cyst wall, and cystic contents were aspirated with syringe. (B) Cyst contained soft suction-able yellowish material of creamy consistency. After cyst wall was sutured, marginal cyst dissection was performed although part of cyst wall adhered to other tissue. Contents were removed with no significant spillage into retropelvic cavity.

Fig. 4 Histopatholgic photomicrographs of tailgut cyst showing smooth muscle proliferation (A) and abundant mucoid material lined by both squamous and glandular mucinous epithelium (B). And cystic wall was lined with transition zone of keratinized squamous, and glandular epithelium, columnar cell involving intracytoplasmic mucin on hematoxylin-eosin stained sections (×100).
Reference
-
1. Lim SW, Huh JW, Kim YJ, Kim HR. Laparoscopy-assisted resection of tailgut cysts: report of a case. Case Rep Gastroenterol. 2011; 5:22–27.2. Lin C, Jin K, Lan H, Teng L, Lin J, Chen W. Surgical management of retrorectal tumors: a retrospective study of a 9-year experience in a single institution. Onco Targets Ther. 2011; 4:203–208.3. Neale JA. Retrorectal tumors. Clin Colon Rectal Surg. 2011; 24:149–160.4. Jao SW, Beart RW Jr, Spencer RJ, Reiman HM, Ilstrup DM. Retrorectal tumors. Mayo Clinic experience, 1960-1979. Dis Colon Rectum. 1985; 28:644–652.5. Hassan I, Wietfeldt ED. Presacral tumors: diagnosis and management. Clin Colon Rectal Surg. 2009; 22:84–93.6. Ghosh J, Eglinton T, Frizelle FA, Watson AJ. Presacral tumours in adults. Surgeon. 2007; 5:31–38.7. Rosa G, Lolli P, Vergine M, El-Dalati G, Malleo G. Surgical excision of developmental retrorectal cysts: results with longterm follow-up from a single institution. Updates Surg. 2012; 64:279–284.8. Charalampakis V, Stamatiou D, Christo-doulakis M, Kafousi M, Chryssou E, de Bree E, et al. Large presacral tailgut cyst with a carcinoid tumor in a male: report of a case. Surg Today. 2014; 44:961–966.9. Kildusis E, Samalavicius NE. Surgical management of a retro-rectal cystic hamartoma (tailgut cyst) using a trans-rectal approach: a case report and review of the literature. J Med Case Rep. 2014; 8:11.10. Mitsuyama T, Kubota M, Nakamura Y, Yuzurihara M, Hoshi K, Okada Y. Neuroendocrine tumor arising from tailgut cyst with spinal cord tethering: case report and literature review. Spine J. 2015; 15:e1–e8.
