Posterior Body Surface Potential Mapping Using Capacitive-Coupled Electrodes and Its Application
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea. seil@snu.ac.kr
- 2Interdisciplinary Program for Bioengineering, Seoul National University, Seoul, Korea.
- 3Department of Biomedical Engineering, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2157975
- DOI: http://doi.org/10.3346/jkms.2012.27.12.1517
Abstract
- Using 49 capacitive-coupled electrodes, mattress-type harness was developed to obtain posterior body surface potential map (P-BSPM) in dressed individuals. The aim of this study was to investigate how valuable information P-BSPM could provide, especially in discrimination of old myocardial infarction (OMI). P-BSPM of 59 individuals were analyzed; 23 normal control, 11 right bundle branch block (RBBB), 3 left bundle branch block (LBBB) and 19 OMI patients. Principal component analysis and linear hyper-plane approach were used to evaluate diagnostic performance. The axes of P-BSPM vector potential corresponded well with 12-lead electrocardiogram. During QRS, the end point of P-BSPM vector potential demonstrated characteristic clockwise rotation in RBBB, and counterclockwise rotation in LBBB patients. In OMI, initial negativity on P-BSPM during QRS was more frequently located at lower half, and also stronger in patients with inferior myocardial infarction (MI). The area under the receiver-operating characteristic curve of P-BSPM during QRS in diagnosing overall OMI, anterior MI, and inferior MI was 0.83 (95% confidence interval, 0.70-0.97), 0.71 (0.47-0.94), and 0.98 (0.94-1.0), respectively (P = 0.022 for anterior vs inferior MI groups). In conclusion, the novel P-BSPM provides detailed information for cardiac electrical dynamics and is applicable to diagnosing OMI, especially inferior myocardial infarction.
MeSH Terms
Figure
-

Fig. 1 Posterior body surface potential mapping (P-BSPM) system. (A) Geometry of capacitive-coupled electrode including preamp, insulator, electrode face and shielding case. (B) Photograph of the mattress-type P-BSPM harness.
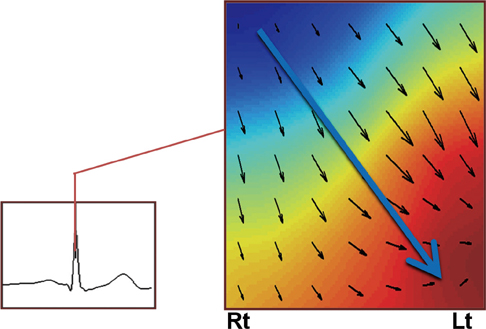
Fig. 2 Example of P-BSPM isopotential map and its vector potential. Potential increases from blue to red color. Small black arrows represent potential gradient vector at each electrode, which sum to vector potential of P-BSPM, the large blue arrow. Rt, right; Lt, left.
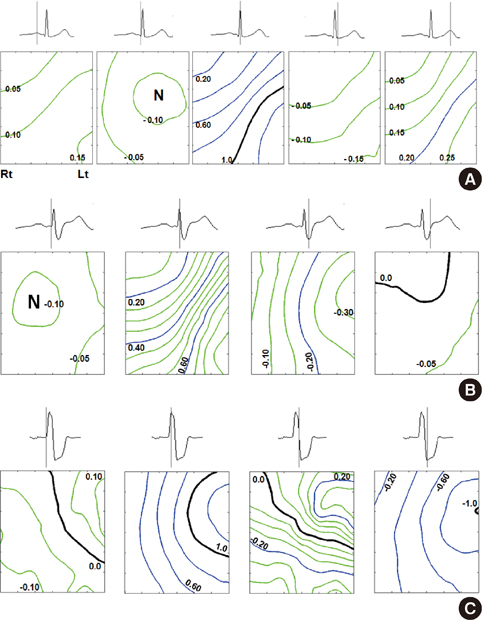
Fig. 3 Averaged iso-potential P-BSPM at specific time. (A) Normal control, (B) right bundle branch block, and (C) left bundle branch block group. Potential interval is 0.05, 0.20, and 1.0 between green, blue, and black lines, respectively. N indicates minimum negativity on the map.

Fig. 4 Representative tracing of vector potential during QRS. (A) Normal control, (B) right bundle branch block, and (C) left bundle branch block patients. The end point of vector was displayed in 3D-cylindrical coordinate, with averaged potential of 49 electrodes as z-axis. Each circle on the line represents 5 ms time interval and darker circles indicates later events.

Fig. 5 Locations of initial negativities during the ventricular depolarization normal control, anterior MI, and inferior MI groups. Four patients of anterior MI group had no negativity, and excluded from this plotting. NC, normal control; MI, myocardial infarction.
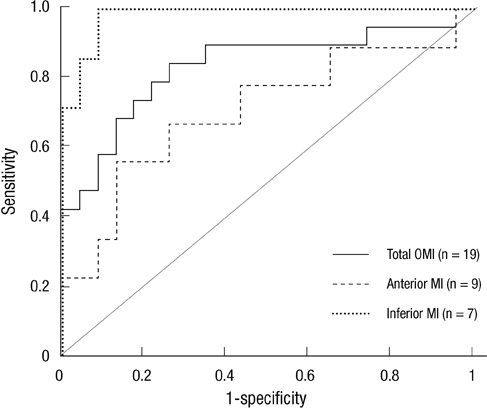
Fig. 6 Receiver-operating characteristic curves of P-BSPM during the QRS in diagnosing OMI. The method of the linear hyperplane approach and the principal component analysis was used. Area under the curve was 0.83 (95% confidence interval, 0.70-0.97), 0.71 (0.47-0.94), and 0.98 (0.94-1.0) for total OMI, anterior MI, and inferior MI group, respectively. OMI, old myocardial infarct; MI, myocardial infarction.
Reference
-
1. Maynard SJ, Menown IB, Manoharan G, Allen J, McC Anderson J, Adgey AA. Body surface mapping improves early diagnosis of acute myocardial infarction in patients with chest pain and left bundle branch block. Heart. 2003. 89:998–1002.2. McClelland AJ, Owens CG, Menown IB, Lown M, Adgey AA. Comparison of the 80-lead body surface map to physician and to 12-lead electrocardiogram in detection of acute myocardial infarction. Am J Cardiol. 2003. 92:252–257.3. Suzuki A, Hirai M, Hayashi H, Tomita Y, Ichihara Y, Adachi M, Oguchi S, Takatsu F. The ability of QRST isointegral maps to detect myocardial infarction in the presence of simulated left bundle branch block. Eur Heart J. 1993. 14:1094–1101.4. Libby P. Braunwald's heart disease: a textbook of cardiovascular medicine. 2008. 8th ed. Philadelphia: Saunders/Elsevier.5. Strauss DG, Selvester RH, Lima JA, Arheden H, Miller JM, Gerstenblith G, Marbán E, Weiss RG, Tomaselli GF, Wagner GS, et al. ECG quantification of myocardial scar in cardiomyopathy patients with or without conduction defects: correlation with cardiac magnetic resonance and arrhythmogenesis. Circ Arrhythm Electrophysiol. 2008. 1:327–336.6. Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK, Pennell DJ, Rumberger JA, Ryan T, Verani MS. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart: a statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation. 2002. 105:539–542.7. Lim YG, Kim KK, Park KS. ECG measurement on a chair without conductive contact. IEEE Trans Biomed Eng. 2006. 53:956–959.8. Jolliffe IT. Principal component analysis. 2002. 2nd ed. New York: Springer;xxix. 487.9. Donnelly MP, Nugent CD, Finlay DD, Rooney NF, Black ND. Diagnosing old MI by searching for a linear boundary in the space of principal components. IEEE Trans Inf Technol Biomed. 2006. 10:476–483.10. Green LS, Lux RL, Haws CW, Williams RR, Hunt SC, Burgess MJ. Effects of age, sex, and body habitus on QRS and ST-T potential maps of 1100 normal subjects. Circulation. 1985. 71:244–253.11. Donis V, Guillem MS, Climent AM, Castells F, Chorro FJ, Millet J. Improving the diagnosis of bundle branch block by analysis of body surface potential maps. J Electrocardiol. 2009. 42:651–659.12. Polak-Jonkisz D, Laszki-Szczachor K, Purzyc L, Zwoliñska D, Musial K, Pilecki W, Rusiecki L, Janocha A, Kalka D, Sobieszczañska M. Usefulness of body surface potential mapping for early identification of the intraventricular conduction disorders in young patients with chronic kidney disease. J Electrocardiol. 2009. 42:165–171.13. Kornreich F, Montague TJ, Rautaharju PM. Body surface potential mapping of ST segment changes in acute myocardial infarction. Implications for ECG enrollment criteria for thrombolytic therapy. Circulation. 1993. 87:773–782.14. Kornreich F, Montague TJ, Rautaharju PM. Identification of first acute Q wave and non-Q wave myocardial infarction by multivariate analysis of body surface potential maps. Circulation. 1991. 84:2442–2453.15. Self WH, Mattu A, Martin M, Holstege C, Preuss J, Brady WJ. Body surface mapping in the ED evaluation of the patient with chest pain: use of the 80-lead electrocardiogram system. Am J Emerg Med. 2006. 24:87–112.16. Thygesen K, Alpert JS, White HD, Jaffe AS, Apple FS, Galvani M, Katus HA, Newby LK, Ravkilde J, Chaitman B, et al. Universal definition of myocardial infarction. Circulation. 2007. 116:2634–2653.17. Moller CS, Byberg L, Sundstrom J, Lind L. T wave abnormalities, high body mass index, current smoking and high lipoprotein (a) levels predict the development of major abnormal Q/QS patterns 20 years later. A population-based study. BMC Cardiovasc Disord. 2006. 6:10.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Unusual Angular Arrangement of Electrodes in Capacitive Heating Device: Thermal Distribution and Clinical Application
- Treatment of Delayed Union of Tibial Fracture with Non - invasive Capacitive Coupled Electrical Field
- Development and Thermal Distribution of An RF Capacitive Heating Device
- Thermal Distribution in a Phantom Using 8MHz RF Capacitive Type Hyperthermia
- IdMapper: A Java Application for ID Mapping across Multiple Cross-referencing Providers
