J Korean Med Sci.
2006 Aug;21(4):761-764. 10.3346/jkms.2006.21.4.761.
Myxedema Ascites: Case Report and Literature Review
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea. chs@catholic.ac.kr
- 2Department of Pathology, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 2157836
- DOI: http://doi.org/10.3346/jkms.2006.21.4.761
Abstract
- Myxedema ascites caused by hypothyroidism is rare, so its diagnosis is often delayed and patients frequently receive unnecessary procedures such as liver biopsies and exploratory laparotomies. We report a 71-yr-old man with clinical ascites that was the first manifestation of hypothyroidism, and which resolved completely in response to thyroid hormone replacement therapy. To our knowledge, this is the first report of myxedema ascites in Korea. A review of the literature revealed 51 well-documented cases of myxedema ascites. Analyses of ascites from patients in this condition usually show high protein (>2.5 g/dL) and low white blood cell counts, with a high proportion of lymphocytes. A consistent feature is the good response to thyroid hormone replacement therapy, which has always led to resolution of the ascites. Myxedema ascites is thus rare but easy to treat; it should be borne in mind, especially if the ascites fluid has a high protein content.
Keyword
MeSH Terms
Figure
-

Fig. 1 CT of the abdomen showing massive ascites and normal-sized liver and spleen.

Fig. 2 Microscopic finding of the liver showing accumulation of yellow bile pigment in the hepatocytes (H&E, ×400).
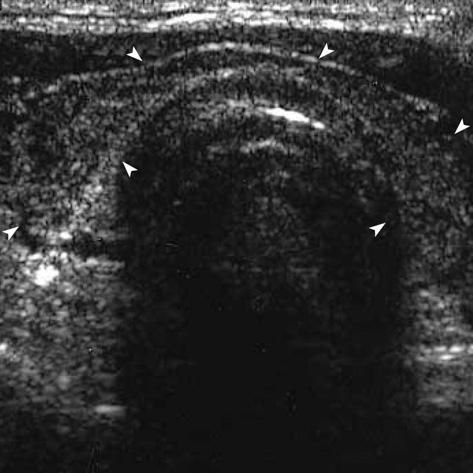
Fig. 3 Thyroid ultrasonograph revealing atrophic change of both thyroid lobes (arrowheads).
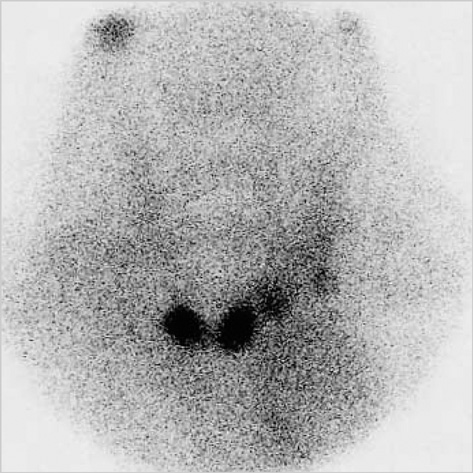
Fig. 4 Technetium-99m thyroid scan showing only two small nodular foci in the thyroid bed.
Reference
-
1. Watanakunakorn C, Hodges RE, Evans TC. Myxedema: a study of 400 cases. Arch Intern Med. 1965. 116:183–190.2. McDonough CH, Lee L, de Beur SJ, Arai S, Vogelsang GB. Myxedema ascites in the posttransplant setting: case report. Am J Hematol. 2002. 71:216–218.
Article3. De Feudis L, Scudieri M, Orlando D, Traisci G. Ascites as preeminent manifestation of primary hypothyroidism: clinical case. Ann Ital Med Int. 1999. 14:294–297.4. Hoefs JC. Serum protein concentration and portal pressure determine the ascitic fluid protein concentration in patient with chronic liver disease. J Lab Clin Med. 1983. 102:260–273.5. Rector WG Jr, Reynolds TB. Superiority of the serum-ascites albumin difference over the ascites total protein concentration in separation of "transudative" and "exudative" ascites. Am J Med. 1984. 77:83–85.
Article6. Hoefs JC. Diagnostic paracentesis: a potent clinical tool. Gastroenterology. 1990. 98:230–236.7. de Castro F, Bonacini M, Walden JM, Schubert TT. Myxedema ascites: report of two cases and review of the literature. J Clin Gastroenterol. 1991. 13:411–414.
Article8. Otero Bedoya J, Landeira G, Corino M, Tamashiro A, Fassio E. Ascites due to hypothyroidism in a patient with alcoholic cirrhosis. Acta Gastroenterol Latinoam. 2001. 31:77–81.9. Runyon BA. Care of patients with ascites. N Engl J Med. 1994. 330:337–342.
Article10. Chiprut RO, Knudsen KB, Liebermann TR, Dyck WP. Myxedema ascites. Am J Dig Dis. 1976. 21:807–808.
Article11. Hazard J, Merot J, Klotz A, Potel M. Ascites revealing thyroid deficiency. Ann Med Interne. 1969. 120:755–759.12. Kinney EL. Myxedema ascites. Am Fam Physician. 1987. 36:134.13. Kocen RS, Atkinson M. Ascites in hypothyroidism. Lancet. 1963. 1:527–530.
Article14. Leung FW, Nortman DF, Shinaberger JH. Myxedema ascites in a patient undergoing chronic hemodyalisis. Dyalisis Transplant. 1982. 11:708–709.15. Madenberg F, Byfield GV, Baker LA. Occurrence of ascites in myxedema. Arch Intern Med. 1954. 93:787–795.
Article16. Desrame J, Mathurin P, Rozov R, Sabate JM, Poynard T, Opolon P, Denis J. Isolated ascites revealing a hypothyroidism: study of 2 cases. Gastroenterol Clin Biol. 1998. 22:732–735.17. Skinner J. Mixedema with thyroid antibodies presenting with ascites. Proc R Soc Med. 1962. 55:997.18. Turner JA, Rapoport J. Mixedema ascites. Postgrad Med J. 1977. 53:343–344.19. Von Knorring J, Friman C. Mechanism of myxedema formation. N Engl J Med. 1980. 302:469.20. Alberti LE, Lopez-Gomez A, Alberti-Flor JJ. Spontaneous bacterial peritonitis in a patient with myxedema ascites. Digestion. 2003. 68:91–93.
Article21. Parving HH, Hansen JM, Nielsen SL, Rossing N, Munck O, Lassen NA. Mechanisms of edema formation in myxedema increased protein extravasation and relatively slow lymphatic drainage. N Engl J Med. 1979. 301:460–465.22. Bonvalet JP, David R, Baglin A, Hatt PY. Myxedema with inappropriate antidiuresis and hyperaldosteronism. Ann Med Interne. 1970. 121:949–955.
