Intraabdominal Cryptococcal Lymphadenitis in a Patient with Systemic Lupus Erythematosus
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Kangnam St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. rapark@catholic.ac.kr
- 2Konkuk University, Seoul, Korea.
- KMID: 2157762
- DOI: http://doi.org/10.3346/jkms.2005.20.6.1059
Abstract
- Cryptococcal infection is a rare, yet well recognized complication of systemic lupus erythematosus (SLE). We present a case of mesenteric and retroperitoneal cryptococcal lymphadenitis resulting in the obstruction of the stomach and proximal duodenum in a patient suffering from SLE, while recently she did not receive any immunosuppressive treatment. A 42-yr-old woman was admitted due to high fever and diffuse abdominal pain for three weeks. Abdominal computed tomography (CT) scan showed multiple conglomerated lymphadenopathies in the retroperitoneum and the mesentery resulting in luminal narrowing of the third portion of the duodenum. Cryptococcal lymphadenitis was proven by needle biopsy and she was treated with intravenous liposomal amphotericin B, followed by oral fluconazole. After fourteen-month antifungal therapies, the clinical symptoms and follow-up images improved. This case emphasize that the intrinsic immunological defects of SLE may be directly responsible for the predisposition to fungal infections.
MeSH Terms
-
Adult
Cryptococcosis/*etiology/pathology/radiography
Female
Humans
Lupus Erythematosus, Systemic/*complications/immunology
Lymphadenitis/*etiology/pathology/radiography
Mesentery
Opportunistic Infections/etiology/pathology/radiography
Research Support, Non-U.S. Gov't
Retroperitoneal Space
Tomography, X-Ray Computed
Figure
-

Fig. 1 Abdominal computed tomography (CT) scan shows the multiple conglomerated soft tissue density lesions noted at the mesenteric root, aortocaval space and left paraaortic space; the CT scan also shows the smooth luminal narrowing noted at the third portion of the duodenum, resulting in marked dilatation of the stomach and proximal duodenum (A). Eight weeks later, the follow up abdominal CT scan shows that there is a marked decrease in the sizes and extents of multiple conglomerated lymphadenopathies in the mesenteric root, aortocaval and left paraaortic space, and the previous noted obstruction of the duodenal third portion is resolved (B).
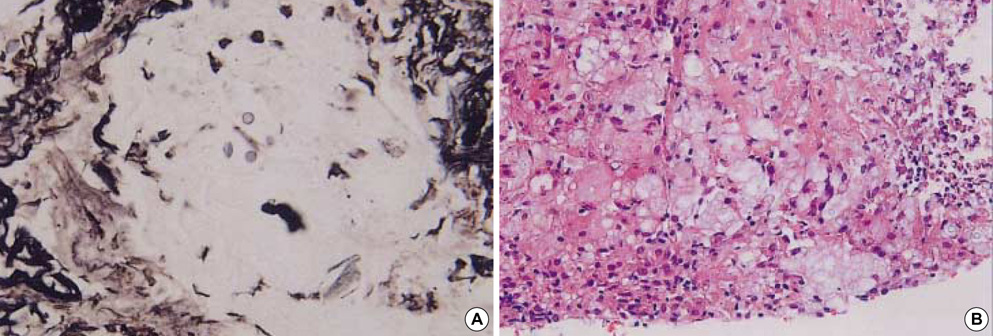
Fig. 2 Under sonographic guidance, percutaneous needle biopsy was performed on the mesenteric conglomerated lymph nodes, and it shows chronic granulomatous inflammation with focal necrosis and a fungal organism: this is consistent with the cryptococcal infection noted on silver staining (A, ×400) and hematoxylin and eosin staining (B, ×100).
Cited by 2 articles
-
Two Cases of Cryptococcuria Developed as Isolated Cryptococcuria and Disseminated Cryptococcosis
Mi Hyun Bae, Seung Namgoong, Dongheui An, Mi-Na Kim, Sung-Han Kim, Ki-Ho Park, Sung-Gyu Lee
Korean J Clin Microbiol. 2011;14(4):148-152. doi: 10.5145/KJCM.2011.14.4.148.A Case of Disseminated Crytococcosis in a Patient with Systemic Lupus Erythematosus
Hye Ryun Jung, Hyun Hee Kwon, Jung-Yoon Choe
J Korean Rheum Assoc. 2010;17(2):194-199. doi: 10.4078/jkra.2010.17.2.194.
Reference
-
1. Abu-Shakra M, Urowitz MB, Gladman DD, Gough J. Mortality studies in systemic lupus erythematosus. Results from a single center. II. Predictor variables for mortality. J Rheumatol. 1995. 22:1265–1270.2. Kang IS, Park SH. Infectious complications in SLE after immunosuppressive therapies. Curr Opin Rheumatol. 2003. 15:528–534.
Article3. Bennet JE. Braunwald E, Fauci AS, Kasper DL, Hauser SL, Longo DL, James JL, editors. Cryptococcosis. Harrison's principles of internal medicine. 2001. 15th ed. New York: McGraw-Hill;1174–1175.4. Lewis JL, Rabinovich S. The wide spectrum of cryptococcal infections. Am J Med. 1972. 53:315–322.
Article5. Eng RH, Bishburg E, Smith SM, Kapila R. Cryptococcal infections in patients with acquired immune deficiency syndrome. Am J Med. 1986. 81:19–23.
Article6. Scalfano FP Jr, Prichard JG, Lamki N, Athey PA, Graces RC. Abdominal cryptococcoma in AIDS: a case report. J Comput Tomogr. 1988. 12:237–239.
Article7. Chong PY, Panabokke RG, Chew KH. Omental cryptococcoma. An unusual presentation of cryptococcosis. Arch Pathol Lab Med. 1986. 110:239–241.8. Mitchell TG, Perfect JR. Cryptococcosis in the era of AIDS: 100 years after the discovery of Cryptococcus neoformans. Clin Microbiol Rev. 1995. 8:515–548.9. Perfect JR, Durack DT, Gallis HA. Cryptococcemia. Medicine (Baltimore). 1983. 62:98–109.
Article10. Miller GP. The immunology of cryptococcal disease. Semin Respir Infec. 1986. 1:45–52.11. Mok CC, Lau CS, Yuen KY. Cryptococcal meningitis presenting concurrently with systemic lupus erythematosus. Clin Exp Rheumatol. 1998. 16:169–171.12. Tsokos GC, Kovacs B, Sfikakis PP, Theocharis S, Vogelgesang S, Via CS. Defective antigen-presenting cell function in patients with systemic lupus erythematosus. Arthritis Rheum. 1996. 39:600–609.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Lupus Erythematosus Profundus Associated with Kikuchi's Disease
- A Case of Disseminated Crytococcosis in a Patient with Systemic Lupus Erythematosus
- A Case of Cryptococcal Meningitis in a Patient with Systemic Lupus Erythematosus
- Cryptococcal Meningitis Presenting with Isolated Sixth Cranial Nerve Palsy in a Patient with Systemic Lupus Erythematosus
- Cryptococcal Meningoencephalitis in a Systemic Lupus Erythematosus Patient without Immunosuppressants
