Combined Use of Automatic Tube Voltage Selection and Current Modulation with Iterative Reconstruction for CT Evaluation of Small Hypervascular Hepatocellular Carcinomas: Effect on Lesion Conspicuity and Image Quality
- Affiliations
-
- 1Department of Radiology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan Province 450052, China. jianbogao0307@163.com
- 2Siemens Healthcare China, Beijing 100102, China.
- KMID: 2155522
- DOI: http://doi.org/10.3348/kjr.2015.16.3.531
Abstract
OBJECTIVE
To assess the lesion conspicuity and image quality in CT evaluation of small (< or = 3 cm) hepatocellular carcinomas (HCCs) using automatic tube voltage selection (ATVS) and automatic tube current modulation (ATCM) with or without iterative reconstruction.
MATERIALS AND METHODS
One hundred and five patients with 123 HCC lesions were included. Fifty-seven patients were scanned using both ATVS and ATCM and images were reconstructed using either filtered back-projection (FBP) (group A1) or sinogram-affirmed iterative reconstruction (SAFIRE) (group A2). Forty-eight patients were imaged using only ATCM, with a fixed tube potential of 120 kVp and FBP reconstruction (group B). Quantitative parameters (image noise in Hounsfield unit and contrast-to-noise ratio of the aorta, the liver, and the hepatic tumors) and qualitative visual parameters (image noise, overall image quality, and lesion conspicuity as graded on a 5-point scale) were compared among the groups.
RESULTS
Group A2 scanned with the automatically chosen 80 kVp and 100 kVp tube voltages ranked the best in lesion conspicuity and subjective and objective image quality (p values ranging from < 0.001 to 0.004) among the three groups, except for overall image quality between group A2 and group B (p = 0.022). Group A1 showed higher image noise (p = 0.005) but similar lesion conspicuity and overall image quality as compared with group B. The radiation dose in group A was 19% lower than that in group B (p = 0.022).
CONCLUSION
CT scanning with combined use of ATVS and ATCM and image reconstruction with SAFIRE algorithm provides higher lesion conspicuity and better image quality for evaluating small hepatic HCCs with radiation dose reduction.
Keyword
MeSH Terms
-
Adult
Aged
Aged, 80 and over
Algorithms
Carcinoma, Hepatocellular/*radiography
Contrast Media
Female
Fluoroscopy
Humans
Image Enhancement/*methods
Liver Neoplasms/*radiography
Male
Middle Aged
Prospective Studies
Radiation Dosage
Radiographic Image Interpretation, Computer-Assisted/*methods
Tomography, X-Ray Computed/*methods
Young Adult
Contrast Media
Figure
-
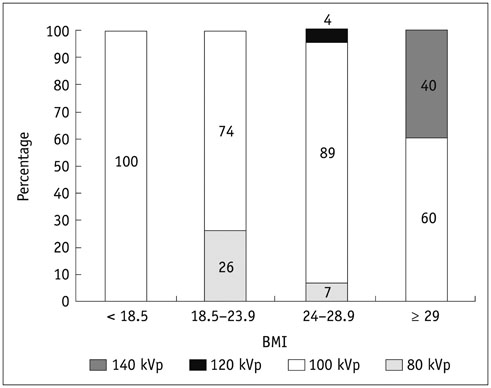
Fig. 1 Distribution of selected tube voltages in group A according to BMI. BMI = body mass indices

Fig. 2 Results of quantitative analysis for all lesions with respect to CNRlesion and image noise among three groups. Among three groups, CNRlesion was highest and image noise was lowest in group A2 (p values ranging from < 0.001 to 0.004). Compared with group B, CNRlesion in group A1 was not significantly different (p > 0.05) while image noise in group A1 was significantly higher (p = 0.002). CNR = contrast-to-noise ratio, HU = Hounsfield unit

Fig. 3 Transverse contrast-enhanced CT images were obtained from 60-year-old man with hepatocellular carcinoma and cirrhosis (BMI, 23.2 kg/m2) (A, B) with combined use of ATVS and ATCM at tube voltage of 100 kVp and from 61-year-old man with hepatocellular carcinoma and cirrhosis using ATCM alone (BMI, 20.6 kg/m2) (C) during LAP. CNR of lesion and mean image noise in group A1 (A), group A2 (B), and group B (C) were as follows: CNR of lesion: 3.60, 4.85, and 4.01; image noise: 10.9, 7.7, and 8.0 HU. ATCM = automatic tube current modulation, ATVS = automatic tube voltage selection, BMI = body mass indices, CNR = contrast-to-noise ratio, HU = Hounsfield unit, LAP = late arterial phase

Fig. 4 Transverse contrast-enhanced CT images were obtained from 50-year-old woman with hepatocellular carcinoma and cirrhosis (BMI, 21.8 kg/m2) (A, B) with combined use of ATVS and ATCM at tube voltage of 80 kVp and from 56-year-old woman with hepatocellular carcinoma and cirrhosis using ATCM alone (BMI, 23.4 kg/m2) (C) during LAP. CNR of lesion and mean image noise in group A1 (A), group A2 (B), and group B (C) were as follows: CNR of lesion: 1.73, 2.61, and 2.15; image noise: 16.9, 11.9, and 9.9 HU. ATCM = automatic tube current modulation, ATVS = automatic tube voltage selection, BMI = body mass indices, CNR = contrast-to-noise ratio, HU = Hounsfield unit, LAP = late arterial phase
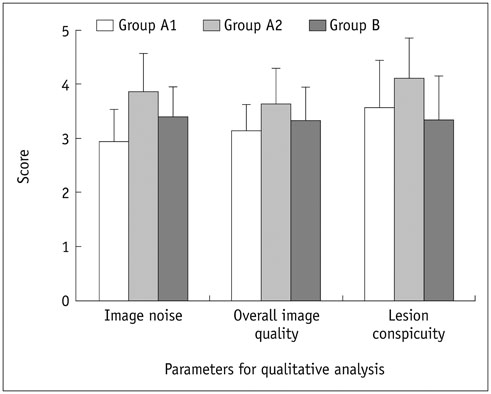
Fig. 5 Results of qualitative analysis for all lesions in terms of image noise, overall image quality, and lesion conspicuity among three groups. Group A2 showed less image noise, and higher overall image quality and lesion conspicuity than group A1 and group B (p values ranging from < 0.001 to 0.001) except for overall image quality between group A2 and group B (p = 0.022). Group B showed less image noise than group A1 (p < 0.001). There was no significant difference in overall image quality and lesion conspicuity between group A1 and group B (p > 0.05).
Cited by 1 articles
-
The Crucial Role of the Establishment of Computed Tomography Density Conversion Tables for Treating Brain or Head/Neck Tumors
Shu-Chin Yang, Su-Hua Lo, Li-Tsuen Shie, Sung-Wei Lee, Sheng-Yow Ho
Prog Med Phys. 2021;32(3):59-69. doi: 10.14316/pmp.2021.32.3.59.
Reference
-
1. Amis ES Jr, Butler PF, Applegate KE, Birnbaum SB, Brateman LF, Hevezi JM, et al. American College of Radiology white paper on radiation dose in medicine. J Am Coll Radiol. 2007; 4:272–284.2. Strzelczyk JJ, Damilakis J, Marx MV, Macura KJ. Facts and controversies about radiation exposure, part 2: low-level exposures and cancer risk. J Am Coll Radiol. 2007; 4:32–39.3. Einstein AJ, Henzlova MJ, Rajagopalan S. Estimating risk of cancer associated with radiation exposure from 64-slice computed tomography coronary angiography. JAMA. 2007; 298:317–323.4. Hall EJ, Brenner DJ. Cancer risks from diagnostic radiology. Br J Radiol. 2008; 81:362–378.5. Hall EJ, Brenner DJ. Cancer risks from diagnostic radiology: the impact of new epidemiological data. Br J Radiol. 2012; 85:e1316–e1317.6. Kramer R, Khoury HJ, Vieira JW. CALDose_X-a software tool for the assessment of organ and tissue absorbed doses, effective dose and cancer risks in diagnostic radiology. Phys Med Biol. 2008; 53:6437–6459.7. Ball CG, Correa-Gallego C, Howard TJ, Zyromski NJ, House MG, Pitt HA, et al. Radiation dose from computed tomography in patients with necrotizing pancreatitis: how much is too much? J Gastrointest Surg. 2010; 14:1529–1535.8. Smith-Bindman R, Lipson J, Marcus R, Kim KP, Mahesh M, Gould R, et al. Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer. Arch Intern Med. 2009; 169:2078–2086.9. Schindera ST, Nelson RC, Yoshizumi T, Toncheva G, Nguyen G, DeLong DM, et al. Effect of automatic tube current modulation on radiation dose and image quality for low tube voltage multidetector row CT angiography: phantom study. Acad Radiol. 2009; 16:997–1002.10. Vardhanabhuti V, Loader R, Roobottom CA. Assessment of image quality on effects of varying tube voltage and automatic tube current modulation with hybrid and pure iterative reconstruction techniques in abdominal/pelvic CT: a phantom study. Invest Radiol. 2013; 48:167–174.11. Siegel MJ, Schmidt B, Bradley D, Suess C, Hildebolt C. Radiation dose and image quality in pediatric CT: effect of technical factors and phantom size and shape. Radiology. 2004; 233:515–522.12. Tamm EP, Rong XJ, Cody DD, Ernst RD, Fitzgerald NE, Kundra V. Quality initiatives: CT radiation dose reduction: how to implement change without sacrificing diagnostic quality. Radiographics. 2011; 31:1823–1832.13. Reid J, Gamberoni J, Dong F, Davros W. Optimization of kVp and mAs for pediatric low-dose simulated abdominal CT: is it best to base parameter selection on object circumference? AJR Am J Roentgenol. 2010; 195:1015–1020.14. Schindera ST, Winklehner A, Alkadhi H, Goetti R, Fischer M, Gnannt R, et al. Effect of automatic tube voltage selection on image quality and radiation dose in abdominal CT angiography of various body sizes: a phantom study. Clin Radiol. 2013; 68:e79–e86.15. Niemann T, Henry S, Faivre JB, Yasunaga K, Bendaoud S, Simeone A, et al. Clinical evaluation of automatic tube voltage selection in chest CT angiography. Eur Radiol. 2013; 23:2643–2651.16. Husarik DB, Schindera ST, Morsbach F, Chuck N, Seifert B, Szucs-Farkas Z, et al. Combining automated attenuationbased tube voltage selection and iterative reconstruction: a liver phantom study. Eur Radiol. 2014; 24:657–667.17. Lee KH, Lee JM, Moon SK, Baek JH, Park JH, Flohr TG, et al. Attenuation-based automatic tube voltage selection and tube current modulation for dose reduction at contrast-enhanced liver CT. Radiology. 2012; 265:437–447.18. Suh YJ, Kim YJ, Hong SR, Hong YJ, Lee HJ, Hur J, et al. Combined use of automatic tube potential selection with tube current modulation and iterative reconstruction technique in coronary CT angiography. Radiology. 2013; 269:722–729.19. Siegel MJ, Hildebolt C, Bradley D. Effects of automated kilovoltage selection technology on contrast-enhanced pediatric CT and CT angiography. Radiology. 2013; 268:538–547.20. Siegel MJ, Ramirez-Giraldo JC, Hildebolt C, Bradley D, Schmidt B. Automated low-kilovoltage selection in pediatric computed tomography angiography: phantom study evaluating effects on radiation dose and image quality. Invest Radiol. 2013; 48:584–589.21. Katsura M, Matsuda I, Akahane M, Yasaka K, Hanaoka S, Akai H, et al. Model-based iterative reconstruction technique for ultralow-dose chest CT: comparison of pulmonary nodule detectability with the adaptive statistical iterative reconstruction technique. Invest Radiol. 2013; 48:206–212.22. Gonzalez-Guindalini FD, Ferreira Botelho MP, Töre HG, Ahn RW, Gordon LI, Yaghmai V. MDCT of chest, abdomen, and pelvis using attenuation-based automated tube voltage selection in combination with iterative reconstruction: an intrapatient study of radiation dose and image quality. AJR Am J Roentgenol. 2013; 201:1075–1082.23. Korn A, Bender B, Fenchel M, Spira D, Schabel C, Thomas C, et al. Sinogram affirmed iterative reconstruction in head CT: improvement of objective and subjective image quality with concomitant radiation dose reduction. Eur J Radiol. 2013; 82:1431–1435.24. Shin HJ, Chung YE, Lee YH, Choi JY, Park MS, Kim MJ, et al. Radiation dose reduction via sinogram affirmed iterative reconstruction and automatic tube voltage modulation (CARE kV) in abdominal CT. Korean J Radiol. 2013; 14:886–893.25. Lv P, Lin XZ, Li J, Li W, Chen K. Differentiation of small hepatic hemangioma from small hepatocellular carcinoma: recently introduced spectral CT method. Radiology. 2011; 259:720–729.26. Kalra MK, Maher MM, Toth TL, Schmidt B, Westerman BL, Morgan HT, et al. Techniques and applications of automatic tube current modulation for CT. Radiology. 2004; 233:649–657.27. Baker ME, Dong F, Primak A, Obuchowski NA, Einstein D, Gandhi N, et al. Contrast-to-noise ratio and low-contrast object resolution on full- and low-dose MDCT: SAFIRE versus filtered back projection in a low-contrast object phantom and in the liver. AJR Am J Roentgenol. 2012; 199:8–18.28. WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004; 363:157–163.29. Rizzo S, Kalra M, Schmidt B, Dalal T, Suess C, Flohr T, et al. Comparison of angular and combined automatic tube current modulation techniques with constant tube current CT of the abdomen and pelvis. AJR Am J Roentgenol. 2006; 186:673–679.30. Lv P, Liu J, Wu R, Hou P, Hu L, Gao J. Use of non-linear image blending with dual-energy CT improves vascular visualization in abdominal angiography. Clin Radiol. 2014; 69:e93–e99.31. Nakaura T, Awai K, Oda S, Funama Y, Harada K, Uemura S, et al. Low-kilovoltage, high-tube-current MDCT of liver in thin adults: pilot study evaluating radiation dose, image quality, and display settings. AJR Am J Roentgenol. 2011; 196:1332–1338.32. Sagara Y, Hara AK, Pavlicek W, Silva AC, Paden RG, Wu Q. Abdominal CT: comparison of low-dose CT with adaptive statistical iterative reconstruction and routine-dose CT with filtered back projection in 53 patients. AJR Am J Roentgenol. 2010; 195:713–719.33. Winklehner A, Goetti R, Baumueller S, Karlo C, Schmidt B, Raupach R, et al. Automated attenuation-based tube potential selection for thoracoabdominal computed tomography angiography: improved dose effectiveness. Invest Radiol. 2011; 46:767–773.34. Yang WJ, Yan FH, Liu B, Pang LF, Hou L, Zhang H, et al. Can sinogram-affirmed iterative (SAFIRE) reconstruction improve imaging quality on low-dose lung CT screening compared with traditional filtered back projection (FBP) reconstruction? J Comput Assist Tomogr. 2013; 37:301–305.35. Kalra MK, Woisetschläger M, Dahlström N, Singh S, Lindblom M, Choy G, et al. Radiation dose reduction with Sinogram Affirmed Iterative Reconstruction technique for abdominal computed tomography. J Comput Assist Tomogr. 2012; 36:339–346.36. Schabel C, Fenchel M, Schmidt B, Flohr TG, Wuerslin C, Thomas C, et al. Clinical evaluation and potential radiation dose reduction of the novel sinogram-affirmed iterative reconstruction technique (SAFIRE) in abdominal computed tomography angiography. Acad Radiol. 2013; 20:165–172.37. Yu MH, Lee JM, Yoon JH, Baek JH, Han JK, Choi BI, et al. Low tube voltage intermediate tube current liver MDCT: sinogramaffirmed iterative reconstruction algorithm for detection of hypervascular hepatocellular carcinoma. AJR Am J Roentgenol. 2013; 201:23–32.38. Hoang JK, Yoshizumi TT, Nguyen G, Toncheva G, Choudhury KR, Gafton AR, et al. Variation in tube voltage for adult neck MDCT: effect on radiation dose and image quality. AJR Am J Roentgenol. 2012; 198:621–627.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effects of Iterative Reconstruction Algorithm, Automatic Exposure Control on Image Quality, and Radiation Dose: Phantom Experiments with Coronary CT Angiography Protocols
- 80-kVp CT Using Iterative Reconstruction in Image Space Algorithm for the Detection of Hypervascular Hepatocellular Carcinoma: Phantom and Initial Clinical Experience
- Feasibility Study of Radiation Dose Reduction in Adult Female Pelvic CT Scan with Low Tube-Voltage and Adaptive Statistical Iterative Reconstruction
- Attenuation-Based Automatic Kilovoltage Selection and Sinogram-Affirmed Iterative Reconstruction: Effects on Radiation Exposure and Image Quality of Portal-Phase Liver CT
- Radiation Dose Reduction via Sinogram Affirmed Iterative Reconstruction and Automatic Tube Voltage Modulation (CARE kV) in Abdominal CT
