Endovascular Treatment of Dural Arteriovenous Fistulas: Single Center Experience
- Affiliations
-
- 1Department of Neurosurgery, Soonchunhyang University Cheonan Hospital, Cheonan, Korea. smyoon@sch.ac.kr
- KMID: 2152914
- DOI: http://doi.org/10.3340/jkns.2016.59.1.17
Abstract
OBJECTIVE
Treatment of intracranial dural arteriovenous fistulas (dAVFs) remains a challenge. However, after introduction of Onyx, transarterial approach is the preferred treatment option in many centers. We report our experience of dAVFs embolization with special emphasis on transarterial approach.
METHODS
Seventeen embolization procedures were performed in 13 patients with dAVFs between Jan 2009 and Oct 2014. Clinical symptoms, location and type of fistulas, embolization methods, complications, radiological and clinical outcomes were evaluated using charts and PACS images.
RESULTS
All 13 patients had symptomatic lesions. The locations of fistulas were transverse-sigmoid sinus in 6, middle fossa dura in 4, cavernous sinus in 2, and superior sagittal sinus in 1 patient. Cognard types were as follows : I in 4, IIa in 2, IIa+IIb in 5, and IV in 2. Embolization procedures were performed > or =2 times in 3 patients. Nine patients were treated with transarterial Onyx embolization alone. One of these required direct surgical puncture of middle meningeal artery. Complete obliteration of fistulas was achieved in 11/13 (85%) patients. There were no complications except for 1 case of Onyx migration in cavernous dAVF. Modified Rankin scale score at post-operative 3 months were 0 in 11, and 3 in 2 patients.
CONCLUSION
Transarterial Onyx embolization can be a first line therapeutic option in patients with dAVFs. However, transvenous approach should be tried first in cavernous sinus dAVF because of the risk of intracranial migration of liquid embolic materials. Furthermore, combined surgical endovascular approach can be considered as a useful option in inaccessible route.
MeSH Terms
Figure
-

Fig. 1 Cerebral angiograms demonstrating complete obliteration of dural arteriovenous fistula (dAVF) using transarterial Onyx embolization in a 56-year-old man. Lateral view of right external carotid artery (ECA) angiograms show a transverse sigmoid sinus dAVF, supplied by multiple feeders from middle meningeal artery (MMA) and occipital artery on early arterial phase (A), and drained retrogradely into an engorged cortical vein on late arterial phase (B). Postoperative lateral view of right ECA angiogram after transarterial injection of 4.5 cc Onyx via petrosal branch of MMA demonstrated complete obliteration of the fistula in single session (C). Postoperative lateral skull radiograph shows the Onyx cast (D).
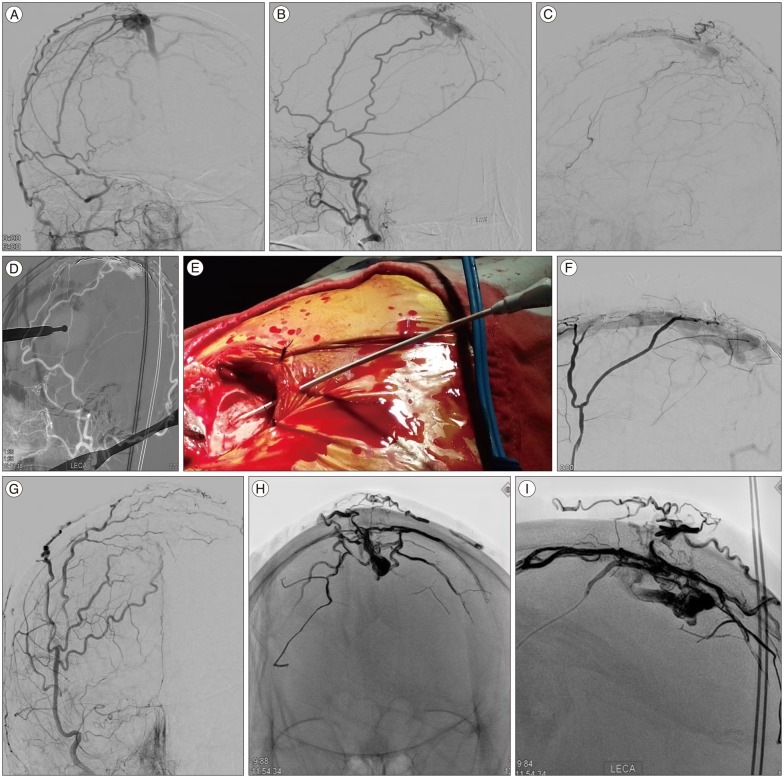
Fig. 2 Transcranial transarterial Onyx embolization of superior sagittal sinus (SSS) dural arteriovenous fistula (dAVF) in a 66-year-old woman. Right external carotid artery (ECA) angiography showed dAVF on superior sagittal sinus (SSS) fed by both middle meningeal arteries (MMAs), superficial temporal arteries (STAs) and occipital arteries (OAs) and drained into the SSS which was occluded in the posterior one third. Marked retrograde bilateral superficial cortical venous reflux was also demonstrated (A and B). Final ECA lateral angiograms of transarterial Onyx embolization through MMA and STA still showed the partial obliteration of dAVF after first session (C). After one week, on second session, roadmap image shows the drilling point of MMA for transcranial transMMA approach (D). Photograph shows the placement of 4 Fr sheath in the MMA and fixation with black silk tie to prevent accidental removal during the procedures (E). Microcatheter angiogram shows the dAVFs clearly (F). Postoperative ECA anterioposterior angiograms showing the complete obliteration of dAVFs without cortical venous reflux (G). Postoperative skull anterioposterior and lateral radiographs shows the Onyx cast after complete obliteration of dAVFs (H and I).

Fig. 3 A case of transvers sigmoid sinus (TSS) dural arteriovenous fistula (dAVF) showing the usefulness of direct sinus exposure. A 72-year-old woman with left TSS dAVF had intractable tinnitus. Brain T2 weighted magnetic resonance image shows the marked low signal intensity on temporo-occipital lobe nearby TSS (A). Left external carotid artery (ECA) lateral angiography shows a left TSS dAVF, supplied by multiple feeders from the ECAs, and draining into the TSS (B). Roadmap anterioposterior image shows that failed transvenous approach because of ipsilateral sinus occlusion and severe stenosis near torcular (C). Although transarterial n-butyle-2-cyanoacrylate embolization was performed through the middle meningeal artery and occipital artery, lateral ECA angiogram shows the partial obliteration on first session (D). Intraoperative photography shows the direct puncture on TSS (E). In the second session, remnant dAVF had successful complete obliteration with transvenous coil embolization through surgically opened and direct punctured on the sinus. And final lateral common carotid angiogram shows the markable obliteration, but remained the a little flow from meningohypophyseal artery (F).
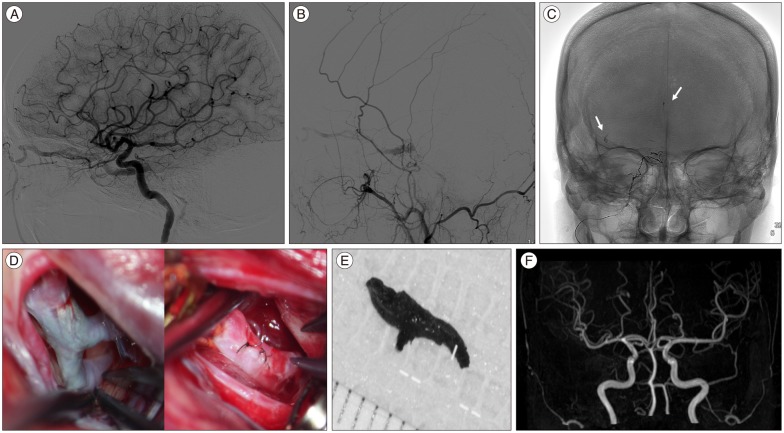
Fig. 4 A complication case showing the risk of Onyx migration in a 49-year-old woman with indirect carotid cavernous fistula. Left internal and external carotid artery angiography shows indirect carotid cavernous fistula, supplied by a feeder from the accessary meningeal artery, and draining into the cavernous sinus (CS) (A and B). Intra-procedural angiogram and skull radiographs shows the migrated Onyx casts (arrows) on intracerebral artery during 0.4 cc Onyx injection (C). Pre and post microsurgical findings of onyx cast removal on middle cerebral artery and photography of removed Onyx cast (D and E). Well recanalized intracerebral artery flow on magnetic resonance angiography (F).
Cited by 3 articles
-
Refractory Spontaneous Chronic Subdural Hematoma: A Rare Presentation of an Intracranial Arteriovenous Fistula
El Kim
J Cerebrovasc Endovasc Neurosurg. 2016;18(4):373-378. doi: 10.7461/jcen.2016.18.4.373.Dural Arteriovenous Fistula Manifested as Rapid Progressive Dementia Successfully Treated by Endovascular Embolization Only
Heewon Hwang, Yun Kyung La, Min Seok Baek, Kyoungwon Baik, Sang Hyun Suh, Won-Joo Kim
Neurointervention. 2017;12(1):50-53. doi: 10.5469/neuroint.2017.12.1.50.Occurrence of
De Novo Dural Arteriovenous Fistula after Transvenous Embolization of Dural Arteriovenous Fistula : Case Reports of Two Patients
Ippei Makita, Yoshinobu Kamio, Hisaya Hiramatsu, Kazuhiko Kurozumi
J Korean Neurosurg Soc. 2022;65(4):598-602. doi: 10.3340/jkns.2021.0144.
Reference
-
1. Awad IA, Little JR, Akarawi WP, Ahl J. Intracranial dural arteriovenous malformations : factors predisposing to an aggressive neurological course. J Neurosurg. 1990; 72:839–850. PMID: 2140125.
Article2. Borden JA, Wu JK, Shucart WA. A proposed classification for spinal and cranial dural arteriovenous fistulous malformations and implications for treatment. J Neurosurg. 1995; 82:166–179. PMID: 7815143.
Article3. Chung SJ, Kim JS, Kim JC, Lee SK, Kwon SU, Lee MC, et al. Intracranial dural arteriovenous fistulas : analysis of 60 patients. Cerebrovasc Dis. 2002; 13:79–88. PMID: 11867880.
Article4. Cognard C, Gobin YP, Pierot L, Bailly AL, Houdart E, Casasco A, et al. Cerebral dural arteriovenous fistulas : clinical and angiographic correlation with a revised classification of venous drainage. Radiology. 1995; 194:671–680. PMID: 7862961.
Article5. Fujita A, Kuwamura K, Saitoh M, Sakagami Y, Takaishi Y, Suzuki S, et al. [Cerebral sinus thrombosis in a patient with protein S deficiency : a case report]. No Shinkei Geka. 1997; 25:467–472. PMID: 9145407.6. Gerlach R, Yahya H, Rohde S, Böhm M, Berkefeld J, Scharrer I, et al. Increased incidence of thrombophilic abnormalities in patients with cranial dural arteriovenous fistulae. Neurol Res. 2003; 25:745–748. PMID: 14579793.
Article7. Hu YC, Newman CB, Dashti SR, Albuquerque FC, McDougall CG. Cranial dural arteriovenous fistula : transarterial Onyx embolization experience and technical nuances. J Neurointerv Surg. 2011; 3:5–13. PMID: 21990779.
Article8. Kerber CW, Newton TH. The macro and microvasculature of the dura mater. Neuroradiology. 1973; 6:175–179. PMID: 4772438.
Article9. Kiyosue H, Hori Y, Okahara M, Tanoue S, Sagara Y, Matsumoto S, et al. Treatment of intracranial dural arteriovenous fistulas : current strategies based on location and hemodynamics, and alternative techniques of transcatheter embolization. Radiographics. 2004; 24:1637–1653. PMID: 15537974.
Article10. Kojima T, Miyachi S, Sahara Y, Nakai K, Okamoto T, Hattori K, et al. The relationship between venous hypertension and expression of vascular endothelial growth factor : hemodynamic and immunohistochemical examinations in a rat venous hypertension model. Surg Neurol. 2007; 68:277–284. discussion 284PMID: 17719966.
Article11. Lv X, Jiang C, Li Y, Wu Z. Results and complications of transarterial embolization of intracranial dural arteriovenous fistulas using Onyx-18. J Neurosurg. 2008; 109:1083–1090. PMID: 19035723.
Article12. Nabors MW, Azzam CJ, Albanna FJ, Gulya AJ, Davis DO, Kobrine AI. Delayed postoperative dural arteriovenous malformations. Report of two cases. J Neurosurg. 1987; 66:768–772. PMID: 3572502.13. Natarajan SK, Ghodke B, Kim LJ, Hallam DK, Britz GW, Sekhar LN. Multimodality treatment of intracranial dural arteriovenous fistulas in the Onyx era : a single center experience. World Neurosurg. 2010; 73:365–379. PMID: 20849795.
Article14. Nogueira RG, Dabus G, Rabinov JD, Eskey CJ, Ogilvy CS, Hirsch JA, et al. Preliminary experience with onyx embolization for the treatment of intracranial dural arteriovenous fistulas. AJNR Am J Neuroradiol. 2008; 29:91–97. PMID: 17974618.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular management of cavernous sinus dural arteriovenous fistulas: Overall review and considerations
- Role of surgery in management of intracranial dural arteriovenous fistulas
- Tentorial Dural Arteriovenous Fistulas: A Single-Center Cohort of 12 Patients
- Stereotactic radiosurgery for dural arteriovenous fistula
- Endovascular Treatment of Dural Sinus Malformation in Infant: A Case Report
