Anomalies of Abdominal Organs in Polysplenia Syndrome: Multidetector Computed Tomography Findings
- Affiliations
-
- 1Department of Radiology, Dongguk University Ilsan Hospital, Dongguk University School of Medicine, Goyang, Korea. yslee@dumc.or.kr
- KMID: 2152603
- DOI: http://doi.org/10.3348/jksr.2016.74.2.114
Abstract
- Polysplenia syndrome is a rare situs ambiguous anomaly associated with multiple spleens and anomalies of abdominal organs. Because most of the minor anomalies do not cause clinical symptoms, polysplenia syndrome is detected incidentally in the adults. Anomalies of abdominal organs may include multiple spleens of variable size or right-sided spleen, large midline or left-sided liver, midline gallbladder, biliary tract anomalies, short pancreas, right-sided stomach, intestinal malrotation, inferior vena cava interruption with azygos or hemiazygos continuation, and a preduodenal portal vein. As the multidetector computed tomography is increasingly used, situs anomalies will likely to be found with greater frequency in the adults. Therefore, radiologists should become familiar with these rare and peculiar anomalies of abdominal organs in polysplenia syndrome.
MeSH Terms
Figure
-
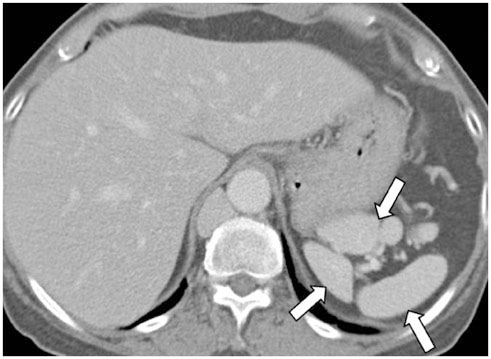
Fig. 1 Polysplenia. Contrast-enhanced axial CT scan shows multiple small discrete splenic tissues (arrows) from the left subphrenic space adjacent to the stomach.
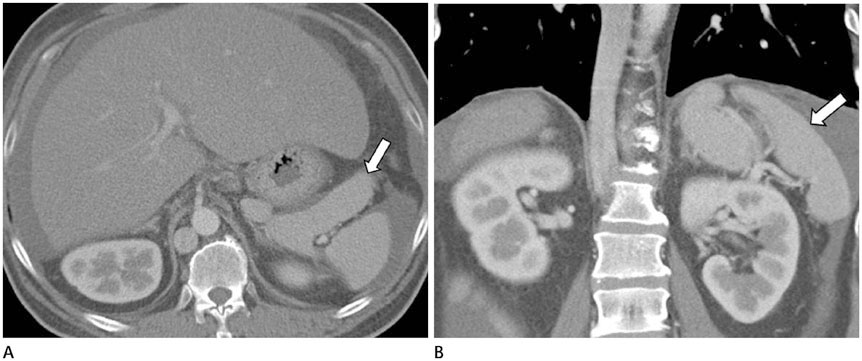
Fig. 2 Polysplenia. Contrast-enhanced axial (A) and coronal reformatted (B) images show several large splenic tissues of lobulating contour (arrows).

Fig. 3 Single spleen. Contrast-enhanced axial (A) and coronal reformatted (B) images show a single small ovoid spleen on the left side (arrows).
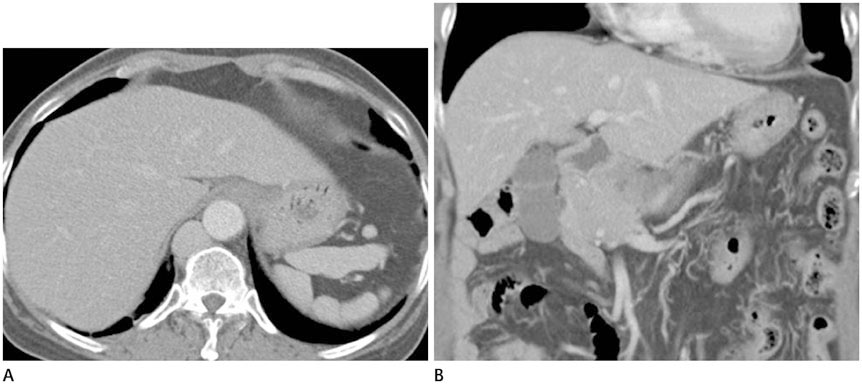
Fig. 4 Location and shape of the liver and gallbladder. Contrast-enhanced axial (A) and coronal reformatted (B) images show a normal location and shape of liver and right-sided gallbladder in a polysplenia patient.
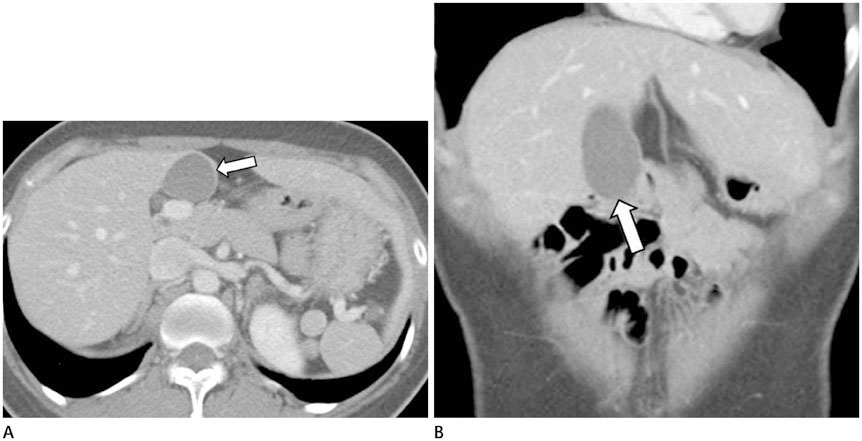
Fig. 5 Midline gallbladder. Contrast-enhanced axial (A) and coronal reformatted (B) images show the midline location of gallbladder (arrows). Although the liver is located on the right side, the left lateral segment is large and located in the left subphrenic space.

Fig. 6 Midline gallbladder and large left lobe of the liver. Contrast-enhanced axial (A, B) and coronal reformatted (C) images show midline location of gallbladder (white arrows). The left lateral segment of the liver is very large (black arrows). Dextrocardia is displayed (black arrowhead) (C).
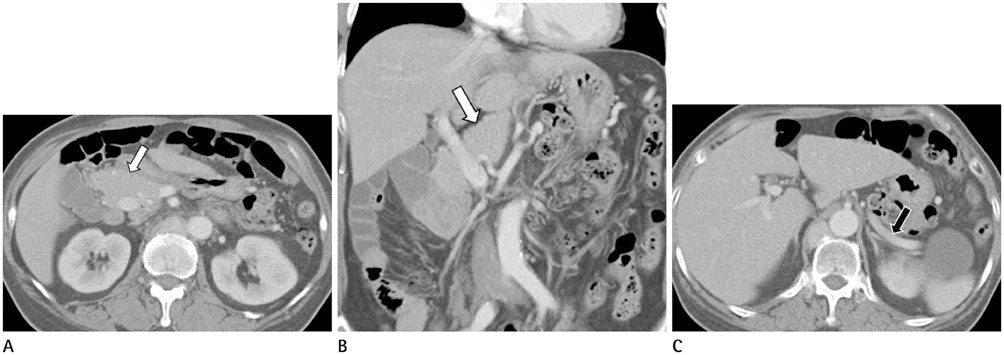
Fig. 7 Short pancreas with agenesis of a dorsal pancreas. Contrast-enhanced axial (A) and coronal reformatted (B) images at the pancreas head level show normal pancreas head (white arrows) developed from the ventral pancreas. Axial CT image at the splenic vein level (C), body and tail of the pancreas is not seen ventral to the splenic vein (black arrow) due to agenesis of the dorsal pancreas.
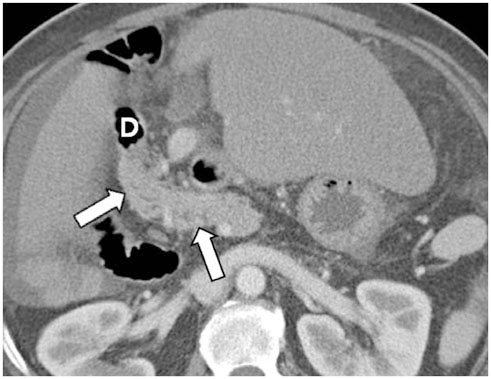
Fig. 8 Right-sided short pancreas. Contrast-enhanced axial CT image shows right-side location of short pancreas head (white arrows). D = duodenum

Fig. 9 Midline short pancreas. Contrast-enhanced axial CT image shows midline location of short pancreas head and body (arrow).
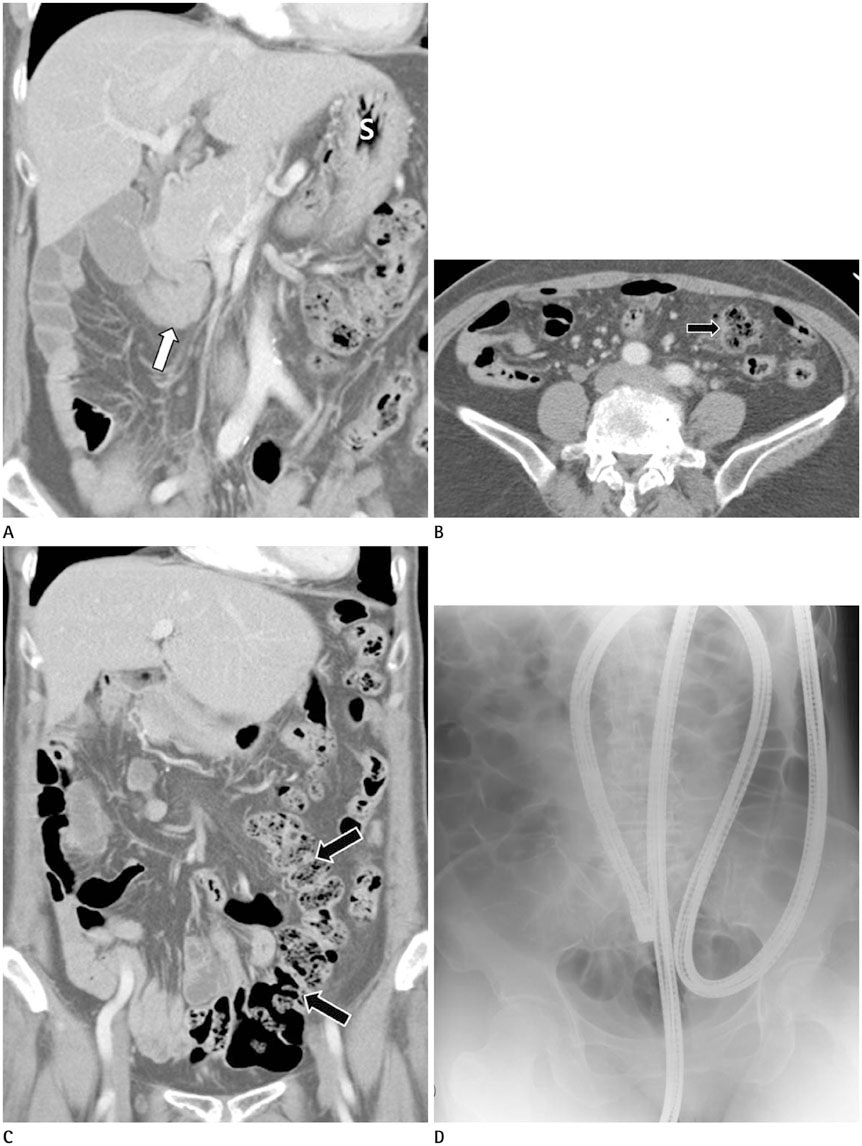
Fig. 10 Intestinal malrotation. A. A contrast-enhanced coronal reformatted CT image. Stomach (S) is located in the left side. Duodenum turns to right side and the duodenojejunal junction (white arrow) is abnormally situated at the right of the midline. B. In the axial image, the ascending colon is found in the left side of abdomen (black arrow). C. In coronal reformatted image, most of the small bowel loops are situated in the right side and the ascending colon is located in the left side of abdomen (black arrows). D. Fluoroscopy during the colonoscopy shows a left-sided colon.
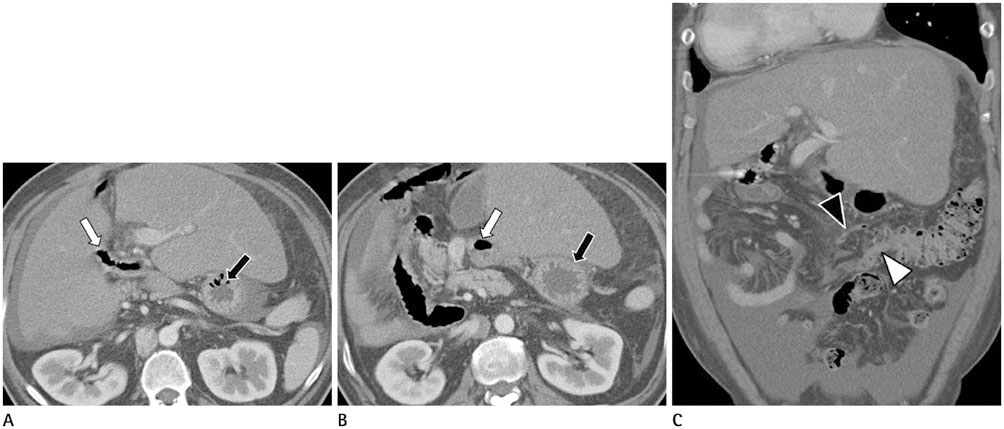
Fig. 11 Intestinal malrotation. A, B. Contrast-enhanced axial images show left side location of the stomach (black arrows). However, the duodenum is directed from left to right side (white arrows). C. A coronal reformatted image shows the left-sided appendix (black arrowhead) and terminal ileum (white arrowhead).
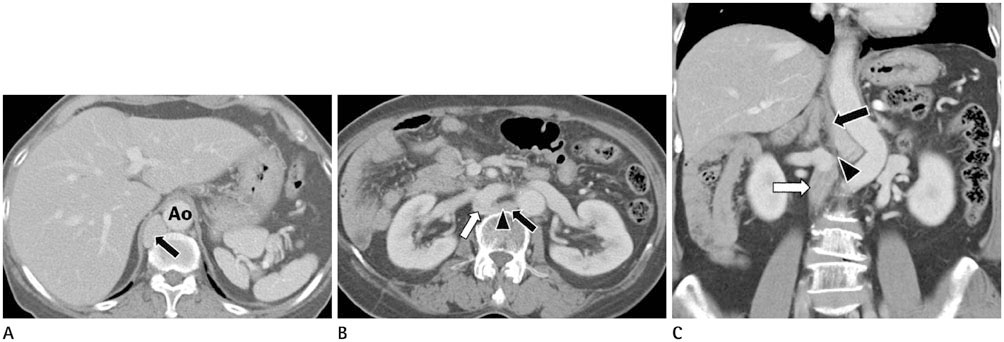
Fig. 12 IVC interruption with azygos continuation. A. Contrast-enhanced axial image shows absence of hepatic segment of the IVC and a dilated azygos vein (arrow) in the retrocrural area adjacent to the descending aorta (Ao). B, C. Axial (B) and coronal reformatted (C) images show interruption of the IVC (white arrows), a dilated azygos vein (black arrows) and the continuation point (arrowheads). IVC = inferior vena cava
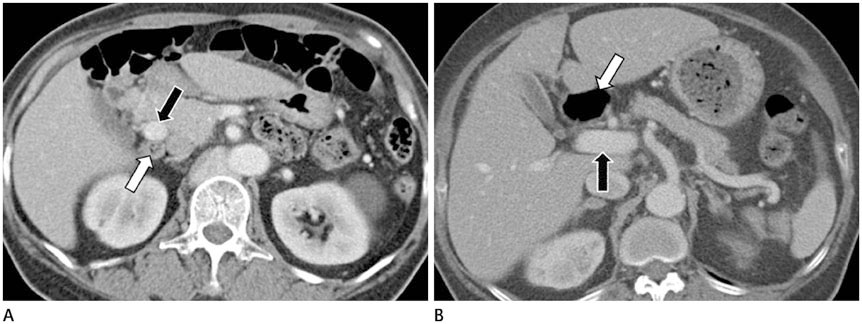
Fig. 13 Preduodenal portal vein. A. On contrast-enhanced axial image, the portal vein (black arrow) traverses anterior to the duodenum (white arrow). B. Normal anatomy for comparison. Duodenum (white arrow) is normally located anterior to the portal vein (black arrow).
Reference
-
1. Muneta S, Sakai S, Fukuda H, Imamura Y, Matsumoto I. Polysplenia syndrome with various visceral anomalies in an adult: embryological and clinical considerations. Intern Med. 1992; 31:1026–1031.2. Fulcher AS, Turner MA. Abdominal manifestations of situs anomalies in adults. Radiographics. 2002; 22:1439–1456.3. Applegate KE, Goske MJ, Pierce G, Murphy D. Situs revisited: imaging of the heterotaxy syndrome. Radiographics. 1999; 19:837–852. discussion 853-8544. Gayer G, Apter S, Jonas T, Amitai M, Zissin R, Sella T, et al. Polysplenia syndrome detected in adulthood: report of eight cases and review of the literature. Abdom Imaging. 1999; 24:178–184.5. Peoples WM, Moller JH, Edwards JE. Polysplenia: a review of 146 cases. Pediatr Cardiol. 1983; 4:129–137.6. Winer-Muram HT, Tonkin IL. The spectrum of heterotaxic syndromes. Radiol Clin North Am. 1989; 27:1147–1170.7. Esscher T. Preduodenal portal vein--a cause of intestinal obstruction? J Pediatr Surg. 1980; 15:609–612.8. Gayer G, Zissin R, Apter S, Atar E, Portnoy O, Itzchak Y. CT findings in congenital anomalies of the spleen. Br J Radiol. 2001; 74:767–772.9. Chandra RS. Biliary atresia and other structural anomalies in the congenital polysplenia syndrome. J Pediatr. 1974; 85:649–655.10. Gagner M, Munson JL, Scholz FJ. Hepatobiliary anomalies associated with polysplenia syndrome. Gastrointest Radiol. 1991; 16:167–171.11. Kobayashi H, Kawamoto S, Tamaki T, Konishi J, Togashi K. Polysplenia associated with semiannular pancreas. Eur Radiol. 2001; 11:1639–1641.12. Maier M, Wiesner W, Mengiardi B. Annular pancreas and agenesis of the dorsal pancreas in a patient with polysplenia syndrome. AJR Am J Roentgenol. 2007; 188:W150–W153.13. Kapa S, Gleeson FC, Vege SS. Dorsal pancreas agenesis and polysplenia/heterotaxy syndrome: a novel association with aortic coarctation and a review of the literature. JOP. 2007; 8:433–437.14. Jeong JH, Kim GH, Song GA, Lee DG, Moon JY, Cheong JH, et al. Polysplenia syndrome with congenital agenesis of dorsal pancreas presenting as acute pancreatitis and the role of endoscopic ultrasonography in its diagnosis. Korean J Gastroenterol. 2012; 60:47–51.15. Rakesh K, Choung OW, Reddy DN. Agenesis of the dorsal pancreas (ADP) and pancreatitis - is there an association? Indian J Gastroenterol. 2006; 25:35–36.16. Nishimori I, Okazaki K, Morita M, Miyao M, Sakamoto Y, Kagiyama S, et al. Congenital hypoplasia of the dorsal pancreas: with special reference to duodenal papillary dysfunction. Am J Gastroenterol. 1990; 85:1029–1033.17. Gold RP. Agenesis and pseudo-agenesis of the dorsal pancreas. Abdom Imaging. 1993; 18:141–144.18. Ditchfield MR, Hutson JM. Intestinal rotational abnormalities in polysplenia and asplenia syndromes. Pediatr Radiol. 1998; 28:303–306.19. Miyabara S, Sugihara H, Kamio A, Oota K, Abe H, Kato S. Atypical polysplenia only with absence of the hepatic segment of inferior vena cava in a middle-aged. Acta Pathol Jpn. 1984; 34:111–116.20. Seo HI, Jeon TY, Sim MS, Kim S. Polysplenia syndrome with preduodenal portal vein detected in adults. World J Gastroenterol. 2008; 14:6418–6420.21. Ishizaki Y, Tanaka M, Okuyama T. Surgical implications of preduodenal portal vein in the adult. Case report and review of the literature. Arch Surg. 1994; 129:773–777.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Absence of the Intrahepatic Inferior Vena Cava with Polysplenia Syndrome on Multidetector Computed Tomography: A Case Report
- Congenital Anomalies of the Aortic Arch: Evaluation with the Use of Multidetector Computed Tomography
- A Case of Scimitar Syndrome with H-Type Tracheoesophageal Fistula and Multiple Anomalies: Diagnosis Using Electrocardiography-Gated Chest CT
- Multidetector CT in Blunt Abdominal Trauma: Imaging Findings and Pitfalls
- Recent Progress in Abdominal CT Imaging
