Clin Endosc.
2015 May;48(3):221-227. 10.5946/ce.2015.48.3.221.
The Efficacy of an Endoscopic Grasp-and-Traction Device for Gastric Endoscopic Submucosal Dissection: An Ex Vivo Comparative Study (with Video)
- Affiliations
-
- 1Department of Gastroenterology and Hepatology, St. Antonius Hospital, Nieuwegein, The Netherlands. d.scholvink@antoniusziekenhuis.nl
- 2Department of Gastroenterology and Hepatology, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands.
- 3Division of Research and Development for Minimally Invasive Treatment, Cancer Center, Keio University School of Medicine, Tokyo, Japan.
- KMID: 2148570
- DOI: http://doi.org/10.5946/ce.2015.48.3.221
Abstract
- BACKGROUND/AIMS
To investigate whether the EndoLifter (Olympus), a counter-traction device facilitating submucosal dissection, can accelerate endoscopic submucosal dissection (ESD).
METHODS
Two endoscopists (novice/expert in ESD) performed 64 ESDs (artificial 3-cm lesions) in 16 ex vivo pig stomachs: per stomach, two at the posterior wall (forward approach) and two at the lesser curvature (retroflex approach). Per approach, one lesion was dissected with (EL+) and one without (EL-) the EndoLifter. The submucosal dissection time (SDT), corrected for specimen size, and the influence of ESD experience on EndoLifter usefulness were assessed.
RESULTS
En bloc resection rate was 98.4%. In the forward approach, the median SDT was shorter with the EndoLifter (0.56 min/cm2 vs. 0.91 min/cm2), although not significantly (p=0.09). The ESD-experienced endoscopist benefitted more from the EndoLifter (0.45 [EL+] min/cm2 vs. 0.68 [EL-] min/cm2, p=0.07) than the ESD-inexperienced endoscopist (0.77 [EL+] min/cm2 vs. 1.01 [EL-] min/cm2, p=0.48). In the retroflex approach, the median SDTs were 1.06 (EL+) and 0.48 (EL-) min/cm2 (p=0.16). The EndoLifter did not shorten the SDT for the ESD-experienced endoscopist (0.68 [EL+] min/cm2 vs. 0.68 [EL-] min/cm2, p=0.78), whereas the ESD-inexperienced endoscopist seemed hindered (1.65 [EL+] min/cm2 vs. 0.38 [EL-] min/cm2, p=0.03).
CONCLUSIONS
In gastric ESD, the EndoLifter, in trend, shortens SDTs in the forward, but not in the retroflex approach. Given the low numbers in this study, a type II error cannot be excluded.
MeSH Terms
Figure
-
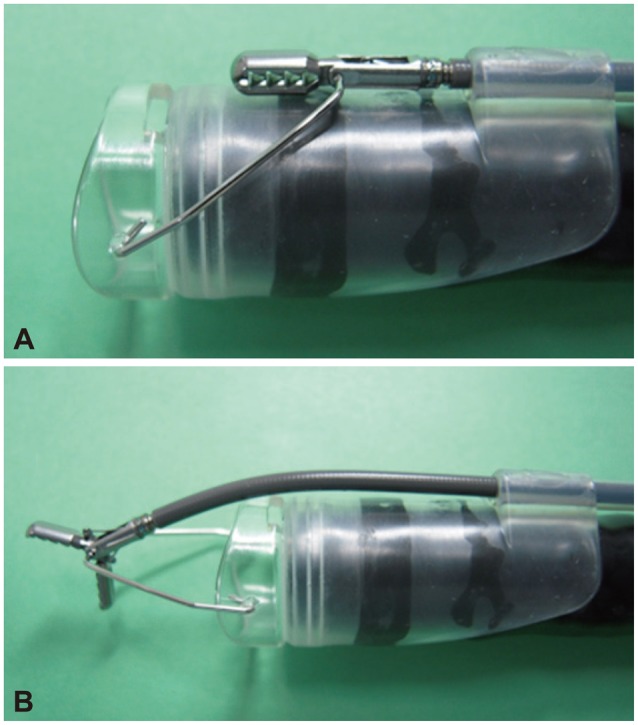
Fig. 1 The EndoLifter (Olympus). (A) The EndoLifter mounted on the tip of an endoscope. (B) Grasping forceps proceeding forward over the tip of the endoscope and opening.
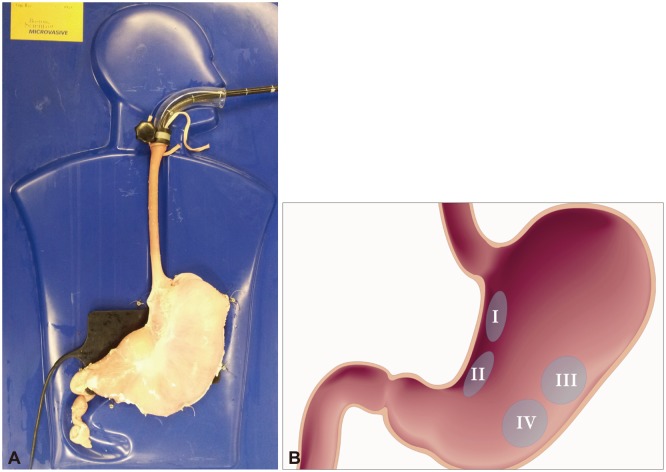
Fig. 2 Experimental set-up. (A) A training kit and the EndoLifter (Olympus). A porcine stomach with the esophagus in a training model, tied with sutures and a glass loop. (B) Per stomach, four artificial lesions (3 cm) are created: I and II at the lesser curvature (retroflex approach) and III and IV at the posterior wall (forward approach).
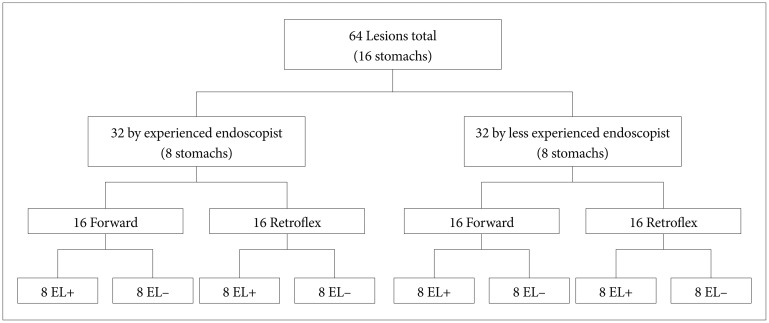
Fig. 3 Experimental set-up II. Flowchart of the study.
Reference
-
1. Pouw RE, Bergman JJ. Endoscopic resection of early oesophageal and gastric neoplasia. Best Pract Res Clin Gastroenterol. 2008; 22:929–943. PMID: 18790439.
Article2. Ribeiro-Mourão F, Pimentel-Nunes P, Dinis-Ribeiro M. Endoscopic submucosal dissection for gastric lesions: results of an European inquiry. Endoscopy. 2010; 42:814–819. PMID: 20886399.
Article3. Ono H, Kondo H, Gotoda T, et al. Endoscopic mucosal resection for treatment of early gastric cancer. Gut. 2001; 48:225–229. PMID: 11156645.
Article4. Yamamoto H, Kawata H, Sunada K, et al. Successful en-bloc resection of large superficial tumors in the stomach and colon using sodium hyaluronate and small-caliber-tip transparent hood. Endoscopy. 2003; 35:690–694. PMID: 12929067.
Article5. Oyama T, Tomori A, Hotta K, et al. Endoscopic submucosal dissection of early esophageal cancer. Clin Gastroenterol Hepatol. 2005; 3(7 Suppl 1):S67–S70. PMID: 16013002.
Article6. Yahagi N, Uraoka T, Ida Y, et al. Endoscopic submucosal dissection using the Flex and the Dual knives. Tech Gastrointest Endosc. 2011; 13:74–78.
Article7. Deprez PH, Bergman JJ, Meisner S, et al. Current practice with endoscopic submucosal dissection in Europe: position statement from a panel of experts. Endoscopy. 2010; 42:853–858. PMID: 20623442.
Article8. Teoh AY, Chiu PW, Hon SF, Mak TW, Ng EK, Lau JY. Ex vivo comparative study using the Endolifter(R) as a traction device for enhancing submucosal visualization during endoscopic submucosal dissection. Surg Endosc. 2013; 27:1422–1427. PMID: 23093235.9. Saito Y, Emura F, Matsuda T, et al. A new sinker-assisted endoscopic submucosal dissection for colorectal cancer. Gastrointest Endosc. 2005; 62:297–301. PMID: 16046999.
Article10. Chen PJ, Chu HC, Chang WK, Hsieh TY, Chao YC. Endoscopic submucosal dissection with internal traction for early gastric cancer (with video). Gastrointest Endosc. 2008; 67:128–132. PMID: 18054010.
Article11. Jeon WJ, You IY, Chae HB, Park SM, Youn SJ. A new technique for gastric endoscopic submucosal dissection: peroral traction-assisted endoscopic submucosal dissection. Gastrointest Endosc. 2009; 69:29–33. PMID: 19111686.
Article12. Li CH, Chen PJ, Chu HC, et al. Endoscopic submucosal dissection with the pulley method for early-stage gastric cancer (with video). Gastrointest Endosc. 2011; 73:163–167. PMID: 21030018.
Article13. Gotoda T, Oda I, Tamakawa K, Ueda H, Kobayashi T, Kakizoe T. Prospective clinical trial of magnetic-anchor-guided endoscopic submucosal dissection for large early gastric cancer (with videos). Gastrointest Endosc. 2009; 69:10–15. PMID: 18599053.
Article14. Sakamoto N, Osada T, Shibuya T, et al. Endoscopic submucosal dissection of large colorectal tumors by using a novel spring-action S-O clip for traction (with video). Gastrointest Endosc. 2009; 69:1370–1374. PMID: 19403131.
Article15. Imaeda H, Iwao Y, Ogata H, et al. A new technique for endoscopic submucosal dissection for early gastric cancer using an external grasping forceps. Endoscopy. 2006; 38:1007–1010. PMID: 16673308.
Article16. Motohashi O, Nishimura K, Nakayama N, Takagi S, Yanagida N. Endoscopic submucosal dissection (two-point fixed ESD) for early esophageal cancer. Dig Endosc. 2009; 21:176–179. PMID: 19691765.
Article17. Yonezawa J, Kaise M, Sumiyama K, Goda K, Arakawa H, Tajiri H. A novel double-channel therapeutic endoscope ("R-scope") facilitates endoscopic submucosal dissection of superficial gastric neoplasms. Endoscopy. 2006; 38:1011–1015. PMID: 17058166.
Article18. Uraoka T, Kato J, Ishikawa S, et al. Thin endoscope-assisted endoscopic submucosal dissection for large colorectal tumors (with videos). Gastrointest Endosc. 2007; 66:836–839. PMID: 17905031.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Is the Endoscopic Grasp-and-Traction Device Useful for Endoscopic Submucosal Dissection in Treating Early Gastric Cancer?
- Debates on Colorectal Endoscopic Submucosal Dissection - Traction for Effective Dissection: Gravity Is Enough
- Efficacy of Current Traction Techniques for Endoscopic Submucosal Dissection
- ESD Hands-on Course Using Ex Vivo and In Vivo Models in South Korea
- Endoscopic Submucosal Dissection in the Treatment of Patients With Papillary Early Gastric Cancer
