Survival and Clinical Behavior of Hypertrophic Cardiomyopathy in a Latin American Cohort in Contrast to Cohorts from the Developed World
- Affiliations
-
- 1Echocardiographic Outpatient Department, National Institute of Cardiology Ignacio Chavez, Mexico City, Mexico.
- 2Cardiology Department, National Institute of Cardiology Ignacio Chavez, Mexico City, Mexico.
- 3Coahuila University, Mexico City, Mexico.
- 4Physiology Department, National Institute of Cardiology Ignacio Chavez, Mexico City, Mexico.
- 5Immunology Department, National Institute of Cardiology Ignacio Chavez, Mexico City, Mexico.
- KMID: 2135402
- DOI: http://doi.org/10.4250/jcu.2015.23.1.20
Abstract
- BACKGROUND
Hypertrophic cardiomyopathy (HCM) is the most common hereditary heart disease with diverse phenotipyc, genetic expession and clinical presentations. The evolution of patients with HCM in Latin America has not been properly described being the frequency, the long-term prognosis as well as the predominant phenotypic expression still unknown. The aim of this study was to determine the survival rate of HCM patients having different phenotypes in a Mexican cohort of patients.
METHODS
Clinical and echocardiographic data obtained from 77 Mexican patients with recently diagnosed HCM were analyzed. The follow-up was of 12.5 years.
RESULTS
96.1% of patients were in functional class I/II according to the New York Heart Association, 2.6% in class III and 1.3% in class IV. Only 3.9% of them went to surgery for myectomy. During the follow-up, 17 patients (22%) died: 4/9 (44%) had apical HCM, 5/20 (25%) had obstructive septal asymmetric HCM, 6/35 (17%) had nonobstructive septal asymmetric HCM and 2/3 (15%) had concentric HCM. The survival rate was worse for patients with apical HCM, followed by those with obstructive and nonobstructive septal asymmetric HCM and patients showing concentric HCM had the best survival rates. There is significant difference in survival rates which declined in 65% in a 9 years-period. Log rank test showed significant differences (p < 0.002).
CONCLUSION
The survival rate of patients with HCM was worse in those with apical variety. The majority of patients received medical treatment. The indication for myectomy was below that observed in other international centers.
MeSH Terms
Figure
-
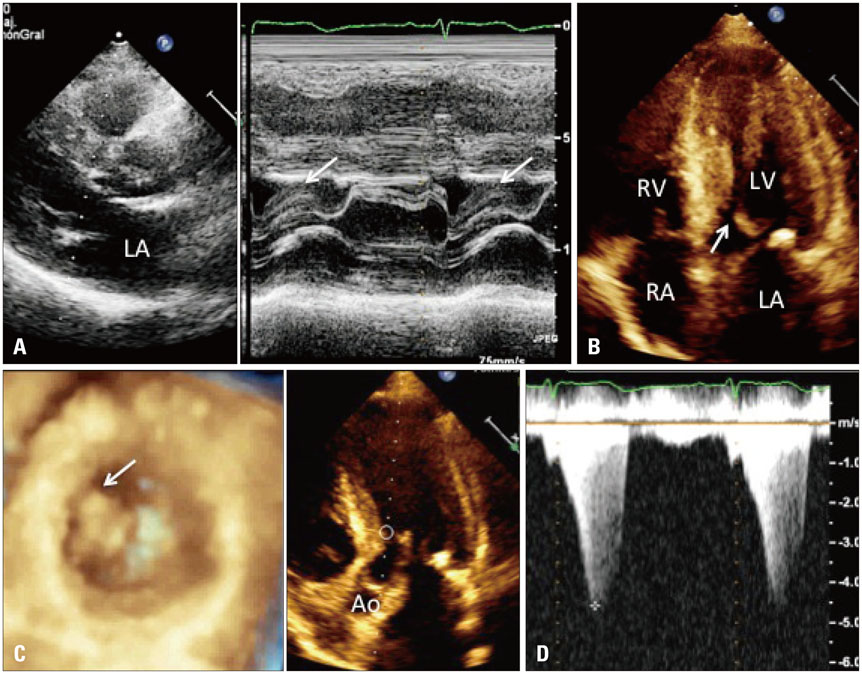
Fig. 1 Parasternal long axis view with M mode (A), two-dimensional apical four-chamber view (B), short axis view at the level of both ventricles (C) and apical 4-chamber view with continuous wave Doppler (D), showing systolic anterior motion of the mitral valve with obstruction of the left ventricle outflow tract (white arrows). The characteristic appearance of the late peak is observed as a dagger. LA: left atrium, LV: left ventricle, RA: right atrium, RV: right ventricle, Ao: aorta.
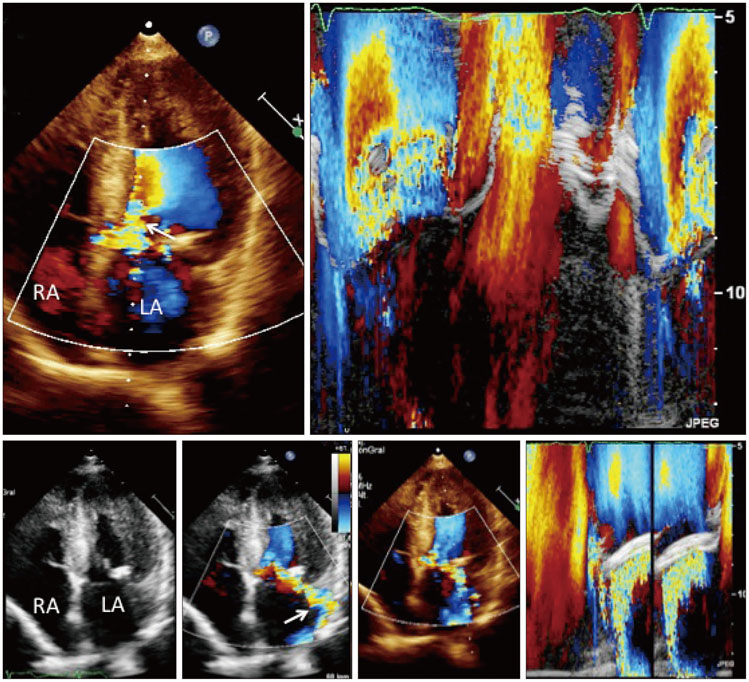
Fig. 2 Two-dimensional echocardiography, M mode and color Doppler of an obstructive septal asymmetric hypertrophic cardiomyopathy. Mitral valve calcification and systolic anterior motion of the mitral valve is observed (white arrow). In the apical 4-chambers view, a dilated left atrium and severe mitral insufficiency is shown (white arrow). LA: left atrium, RA: right atrium.

Fig. 3 Two-dimensional echocardiography in an apical 2 and 4 chambers view, tissue Doppler imaging and tridimensional 4 chamber view, showing apical left ventricular hypertrophy (arrow) and left atrial enlargement. LA: left atrium, LV: left ventricle, RA: right atrium, RV: right ventricle.

Fig. 4 Two-dimensional transthoracic echocardiography in an apical 4 chambers plane and short axis view at the level of both ventricles, showing concentric hypertrophic cardiomyopathy. LA: left atrium, LV: left ventricle, RA: right atrium, RV: right ventricle.
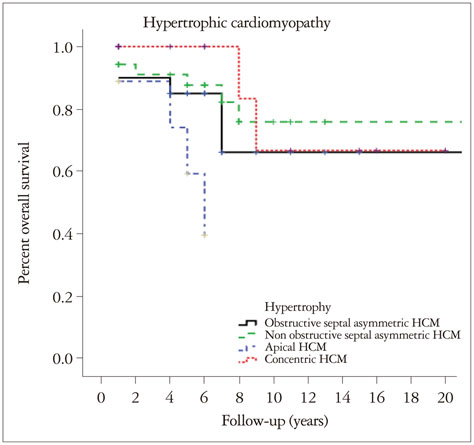
Fig. 5 Actuarial survival curve for the different phenotypes of hyper-trophic cardiomyopathy (HCM) assessed by transthoracic echocardiography in a cohort of Mexican patients from the National Institute of Cardiology "Ignacio Chávez".
Reference
-
1. Maron BJ. Hypertrophic cardiomyopathy: an important global disease. Am J Med. 2004; 116:63–65.2. Kaludercic N, Reggiani C, Paolocci N. Genes, geography and geometry: the "critical mass" in hypertrophic cardiomyopathy. J Mol Diagn. 2009; 11:12–16.3. Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, Link MS, Naidu SS, Nishimura RA, Ommen SR, Rakowski H, Seidman CE, Towbin JA, Udelson JE, Yancy CW. American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2011 ACCF/AHA Guideline for the Diagnosis and Treatment of Hypertrophic Cardiomyopathy: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Developed in collaboration with the American Association for Thoracic Surgery, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2011; 58:e212–e260.4. McKenna W, Deanfield J, Faruqui A, England D, Oakley C, Goodwin J. Prognosis in hypertrophic cardiomyopathy: role of age and clinical, electrocardiographic and hemodynamic features. Am J Cardiol. 1981; 47:532–538.5. Maron BJ, Gardin JM, Flack JM, Gidding SS, Kurosaki TT, Bild DE. Prevalence of hypertrophic cardiomyopathy in a general population of young adults. Echocardiographic analysis of 4111 subjects in the CARDIA Study. Coronary Artery Risk Development in (Young) Adults. Circulation. 1995; 92:785–789.6. Kaple RK, Murphy RT, DiPaola LM, Houghtaling PL, Lever HM, Lytle BW, Blackstone EH, Smedira NG. Mitral valve abnormalities in hypertrophic cardiomyopathy: echocardiographic features and surgical outcomes. Ann Thorac Surg. 2008; 85:1527–1535. 1535.e1–1535.e2.7. Nagueh SF, McFalls J, Meyer D, Hill R, Zoghbi WA, Tam JW, Quiñones MA, Roberts R, Marian AJ. Tissue Doppler imaging predicts the development of hypertrophic cardiomyopathy in subjects with subclinical disease. Circulation. 2003; 108:395–398.8. He XW, Song ZZ. Evaluation of left ventricular function, rotation, twist and untwist in patients with hypertrophic cardiomyopathy. Exp Clin Cardiol. 2013; 18:e47–e49.9. Kimura A, Harada H, Park JE, Nishi H, Satoh M, Takahashi M, Hiroi S, Sasaoka T, Ohbuchi N, Nakamura T, Koyanagi T, Hwang TH, Choo JA, Chung KS, Hasegawa A, Nagai R, Okazaki O, Nakamura H, Matsuzaki M, Sakamoto T, Toshima H, Koga Y, Imaizumi T, Sasazuki T. Mutations in the cardiac troponin I gene associated with hypertrophic cardiomyopathy. Nat Genet. 1997; 16:379–382.10. Bonne G, Carrier L, Richard P, Hainque B, Schwartz K. Familial hypertrophic cardiomyopathy: from mutations to functional defects. Circ Res. 1998; 83:580–593.11. Geisterfer-Lowrance AA, Kass S, Tanigawa G, Vosberg HP, McKenna W, Seidman CE, Seidman JG. A molecular basis for familial hypertrophic cardiomyopathy: a beta cardiac myosin heavy chain gene missense mutation. Cell. 1990; 62:999–1006.12. McKenna WJ, Monserrat Iglesias L. [Sudden death (V). Identification and treatment of patients with hypertrophic cardiomyopathy at risk of sudden death]. Rev Esp Cardiol. 2000; 53:123–130.13. Wigle ED, Rakowski H, Kimball BP, Williams WG. Hypertrophic cardiomyopathy. Clinical spectrum and treatment. Circulation. 1995; 92:1680–1692.14. Maron BJ, Gottdiener JS, Epstein SE. Patterns and significance of distribution of left ventricular hypertrophy in hypertrophic cardiomyopathy. A wide angle, two dimensional echocardiographic study of 125 patients. Am J Cardiol. 1981; 48:418–428.15. Eriksson MJ, Sonnenberg B, Woo A, Rakowski P, Parker TG, Wigle ED, Rakowski H. Long-term outcome in patients with apical hypertrophic cardiomyopathy. J Am Coll Cardiol. 2002; 39:638–645.16. Binder J, Attenhofer Jost CH, Klarich KW, Connolly HM, Tajik AJ, Scott CG, Julsrud PR, Ehrsam JE, Bailey KR, Ommen SR. Apical hypertrophic cardiomyopathy: prevalence and correlates of apical outpouching. J Am Soc Echocardiogr. 2011; 24:775–781.17. Klarich KW, Attenhofer Jost CH, Binder J, Connolly HM, Scott CG, Freeman WK, Ackerman MJ, Nishimura RA, Tajik AJ, Ommen SR. Risk of death in long-term follow-up of patients with apical hypertrophic cardiomyopathy. Am J Cardiol. 2013; 111:1784–1791.18. Woo A, Rakowski H, Liew JC, Zhao MS, Liew CC, Parker TG, Zeller M, Wigle ED, Sole MJ. Mutations of the beta myosin heavy chain gene in hypertrophic cardiomyopathy: critical functional sites determine prognosis. Heart. 2003; 89:1179–1185.19. Ommen SR, Nishimura RA. Hypertrophic cardiomyopathy. Curr Probl Cardiol. 2004; 29:239–291.20. Braunwald E, Seidman CE, Sigwart U. Contemporary evaluation and management of hypertrophic cardiomyopathy. Circulation. 2002; 106:1312–1316.21. Elliott PM, Gimeno JR, Tomé MT, Shah J, Ward D, Thaman R, Mogensen J, McKenna WJ. Left ventricular outflow tract obstruction and sudden death risk in patients with hypertrophic cardiomyopathy. Eur Heart J. 2006; 27:1933–1941.22. Maron MS, Olivotto I, Betocchi S, Casey SA, Lesser JR, Losi MA, Cecchi F, Maron BJ. Effect of left ventricular outflow tract obstruction on clinical outcome in hypertrophic cardiomyopathy. N Engl J Med. 2003; 348:295–303.23. O'Mahony C, Jichi F, Pavlou M, Monserrat L, Anastasakis A, Rapezzi C, Biagini E, Gimeno JR, Limongelli G, McKenna WJ, Omar RZ, Elliott PM. Hypertrophic Cardiomyopathy Outcomes Investigators. A novel clinical risk prediction model for sudden cardiac death in hypertrophic cardiomyopathy (HCM risk-SCD). Eur Heart J. 2014; 35:2010–2020.24. Elliott PM, Poloniecki J, Dickie S, Sharma S, Monserrat L, Varnava A, Mahon NG, McKenna WJ. Sudden death in hypertrophic cardiomyopathy: identification of high risk patients. J Am Coll Cardiol. 2000; 36:2212–2218.25. Arad M, Penas-Lado M, Monserrat L, Maron BJ, Sherrid M, Ho CY, Barr S, Karim A, Olson TM, Kamisago M, Seidman JG, Seidman CE. Gene mutations in apical hypertrophic cardiomyopathy. Circulation. 2005; 112:2805–2811.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Apical Hypertrophic Cardiomyopathy with Apical Aneurysm and Thrombus Diagnosed by Contrast Echocardiography
- Non-invasive Assessment of Hypertrophic Cardiomyopathy
- Tips for Successful Septal Myectomy in Patients with Hypertrophic Cardiomyopathy
- A Case of Normalized Hypertrophic Cardiomyopathy after Removal of Pheochromocytoma
- A Case of Regressed Apical Hypertrophic Cardiomyopathy
