A Case of Giant Skull Base Chondroma
- Affiliations
-
- 1Department of Neurosurgery, Soonchunhyang University Seoul Hospital, Seoul, Korea. chosj@schmc.ac.kr
- KMID: 2134278
- DOI: http://doi.org/10.14791/btrt.2014.2.2.92
Abstract
- Intracranial chondroma is a rare benign tumor. Here, we present the case of a 29-year-old female who was afflicted with left eye blindness and ptosis. Brain computerized tomography and magnetic resonance imaging revealed the presence of a giant calcified mass accompanied by a solid mass in the middle and posterior fossa. A differential diagnosis regarding chordoma, chondrosarcoma, and other chondroid tumors based on radiologic information was inconclusive. The lesion was resected completely under a microscope using a combined pterional and subtemporal approach. The pathologic report confirmed the diagnosis of chondroma. No evidence of neurological worsening was observed. The tumor had a calcified mass with mature hyaline cartilage surrounded by a thick fibrous capsule. We dissected the periphery of the tumor mass and removed it via aspiration. It was readily distinguished from normal brain parenchymal tissue. The large calcified mass at the center of the tumor had relatively high vascularity, and a high-speed drill and various rongeurs were used to remove the tumor.
Keyword
MeSH Terms
Figure
-
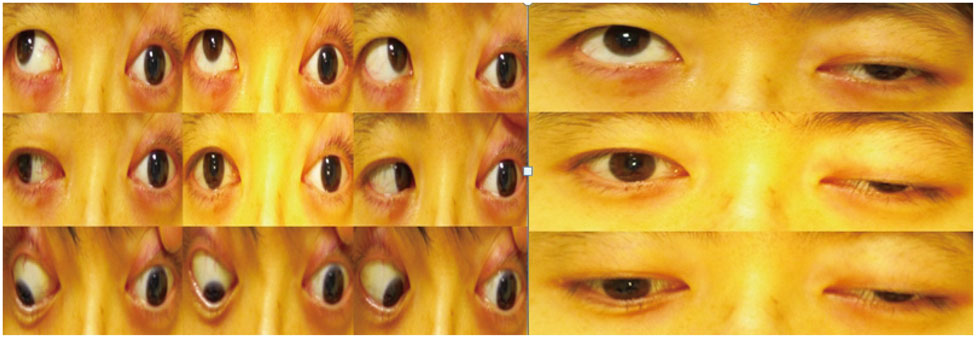
Fig. 1 A 29-year-old female presented with left-side ptosis and a fixed eyeball.
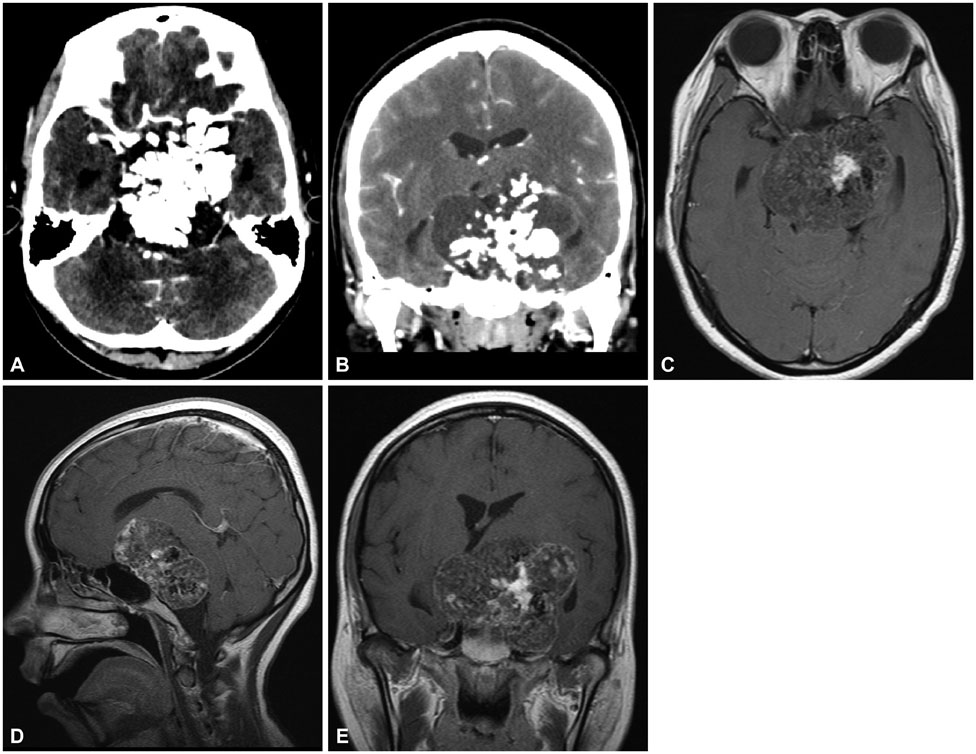
Fig. 2 Computed tomography (CT) revealed a giant high density lesion in the central protion of the mass indicating dense calcification (A and B). Gadolinium-enhanced axial magnetic resonance imaging (MRI) revealed a solitary mass in the prepontine cistern extending to the suprasellar cistern. The lesion showed heterogeneous nonenhancement following the intravenous administration of a gadolinium-based contrast agent. No evidence of peritumoral edema was observed (C, D, and E).

Fig. 3 A Gross specimen consisting of a large calcified mass was obtained from the center of the tumor.
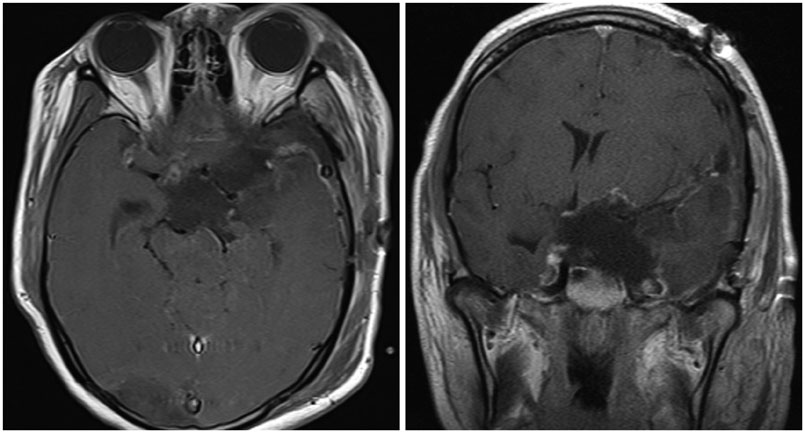
Fig. 4 Postoperative MRI showed that the lesion was completely resected.

Fig. 5 Histological findings. It shows lobular paucicellular proliferation of tumor cells on the myxochondroid background. Each cell has a small hyperchromatic nucleus without atypism.
Reference
-
1. Kurt E, Beute GN, Sluzewski M, van Rooij WJ, Teepen JL. Giant chondroma of the falx. Case report and review of the literature. J Neurosurg. 1996; 85:1161–1164.2. Patel A, Munthali L, Bodi I. Giant cystic intracranial chondroma of the falx with review of literature. Neuropathology. 2009; 29:315–317.
Article3. Pallini R, Lauretti L, Fernandez E, Colosimo C. Giant chondroma of the falx. J Neurosurg. 1997; 87:333–334.4. Mobbs RJ, Narula S, Berger M, Kwok BC. Intracranial chondroma of the occipital lobe. Australas Radiol. 1998; 42:74–76.
Article5. Nakazawa T, Inoue T, Suzuki F, Nakasu S, Handa J. Solitary intracranial chondroma of the convexity dura: case report. Surg Neurol. 1993; 40:495–498.
Article6. De Coene B, Gilliard C, Grandin C, Nisolle JF, Trigaux JP, Lahdou JB. Unusual location of an intracranial chondroma. AJNR Am J Neuroradiol. 1997; 18:573–575.7. Ramamurthi B, Iyer CG, Vedachalam SP. Intracranial meningeal chondroma. J Neurosurg. 1961; 18:826–828.
Article8. Russell DS, Rubinstein LS. Pathology of Tumours of the Nervous System. 2nd ed. London: Edward Arnoid Ltd.;1963.9. Lacerte D, Gagné F, Copty M. Intracranial chondroma. Report of two cases and review of the literature. Can J Neurol Sci. 1996; 23:132–137.
Article10. Nakayama M, Nagayama T, Hirano H, Oyoshi T, Kuratsu J. Giant chondroma arising from the dura mater of the convexity. Case report and review of the literature. J Neurosurg. 2001; 94:331–334.11. Shariat Torbaghan S, Ashouri M, Jalayer Naderi N, Baherini N. Histopathologic Differentiation between Enchondroma and Well-differentiated Chondrosarcoma: Evaluating the Efficacy of Diagnostic Histologic Structures. J Dent Res Dent Clin Dent Prospects. 2011; 5:98–101.12. Eefting D, Schrage YM, Geirnaerdt MJ, et al. Assessment of interobserver variability and histologic parameters to improve reliability in classification and grading of central cartilaginous tumors. Am J Surg Pathol. 2009; 33:50–57.
Article13. Grossman RI, Davis KR. Cranial computed tomographic appearance of chondrosarcoma of the base of the skull. Radiology. 1981; 141:403–408.
Article14. Acampora S, Troisi F, Fusco G, Del Gaizo S. Voluminous intracranial chondroma. Surg Neurol. 1982; 18:254–257.
Article15. Hardy RW Jr, Benjamin SP, Gardner WJ. Prolonged survival following excision of dural chondroma. J Neurosurg. 1978; 48:125–127.
Article16. Mapstone TB, Wongmongkolrit T, Roessman U, Ratcheson RA. Intradural chondroma: a case report and review of the literature. Neurosurgery. 1983; 12:111–114.
Article
