Changes in Arterioportal Shunts in Hepatocellular Carcinoma Patients with Portal Vein Thrombosis Who Were Treated with Chemoembolization Followed by Radiotherapy
- Affiliations
-
- 1Department of Radiation Oncology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. rophc@skku.edu
- 2Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2132803
- DOI: http://doi.org/10.4143/crt.2014.011
Abstract
- PURPOSE
In this study, we retrospectively investigated the prevalence of arterioportal (AP) shunts in hepatocellular carcinoma (HCC) patients with portal vein tumor thrombosis (PVTT) and evaluated the changes in AP shunts after chemoembolization followed by external beam radiation therapy (EBRT).
MATERIALS AND METHODS
We analyzed 54 HCC patients with PVTT who were treated with chemoembolization followed by EBRT. EBRT was uniformly delivered at a total dose of 30 to 45 Gy (median, 35 Gy), with a daily dose of 2 to 4.5 Gy. Angiographic images of chemoembolization before and after radiation therapy (RT) were reviewed to investigate the AP shunt.
RESULTS
During the initial session of chemoembolization, 33 of 54 patients (61%) had an AP shunt. After EBRT, 32 out of 33 patients had an additional session of chemoembolization and were evaluated for a change in the AP shunt. The AP shunt decreased in 20 of 32 patients (63%) after chemoembolization followed by EBRT. The 1-year calculated overall survival (OS) rate for all patients was 52.6% and the 2-year OS was 36.4%. The median OS in all patients was 13 months. Patients with AP shunt showed poorer median OS than those without AP shunt, but there was no statistically significant difference (median, 12 months vs. 17 months).
CONCLUSION
The AP shunt frequently occurs in HCC patients with PVTT. This study suggests that a poor prognosis is associated with an AP shunt. Chemoembolization followed by RT may produce a decrease in AP shunts.
MeSH Terms
Figure
-
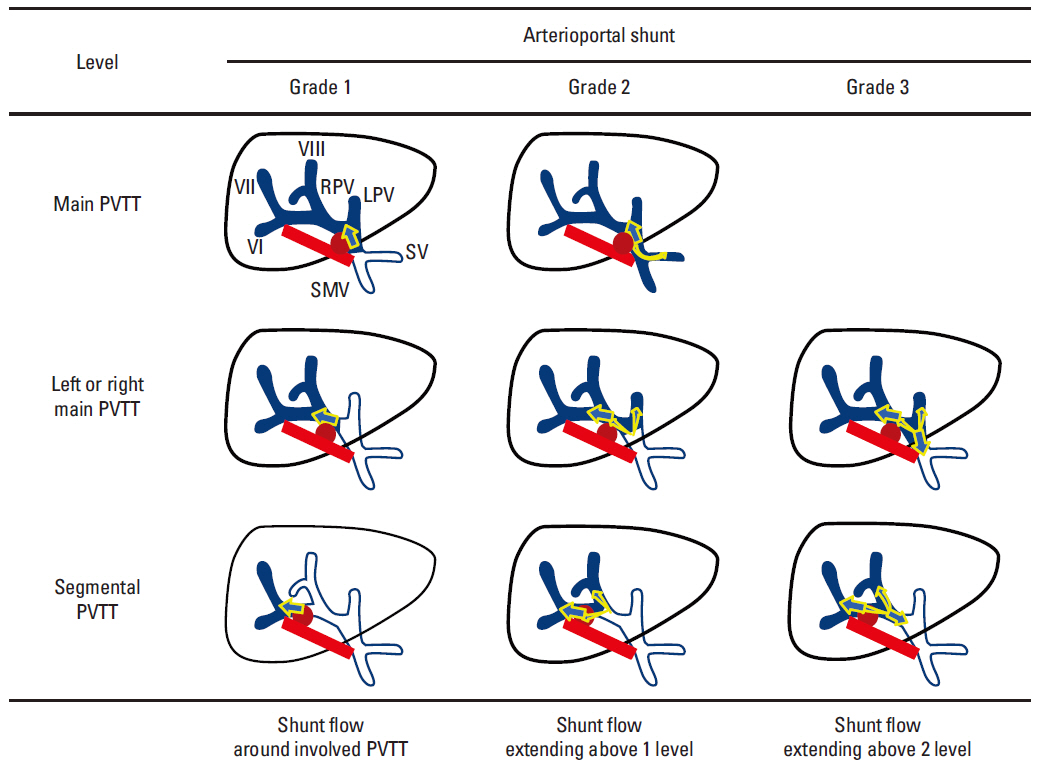
Fig. 1. The grading system for arterioportal shunting flow. PVTT, portal vein tumor thrombosis; SMV, superior mesenteric vein; SV, splenic vein; RPV, right portal vein; LPV, left portal vein; arrow, shunt flow; red circle, tumor; orange line, hepatic artery; blue, portal vein.

Fig. 2. Change in arterioportal (AP) shunt after chemoembolization followed by radiation therapy. (A, B) A 76-year-old patient with left main portal vein tumor thrombus (PVTT) had angiography that showed a grade 2 AP shunt. (A) An AP shunt from the left portal vein (arrow) extends to the right portal vein (arrowhead). (B) After chemoembolization followed by RT, the angiography during the second session of chemoembolization showed minimal shunt flow around the left portal vein (arrow). (C, D) A 56-year-old patient had a S2/4 main tumor and segmental PVTT. (C) The angiography during the first session of chemoembolization showed AP shunt flow to the segmental portal vein (arrows). (D) After chemoembolization followed by RT, the AP shunt flow was completely obliterated.
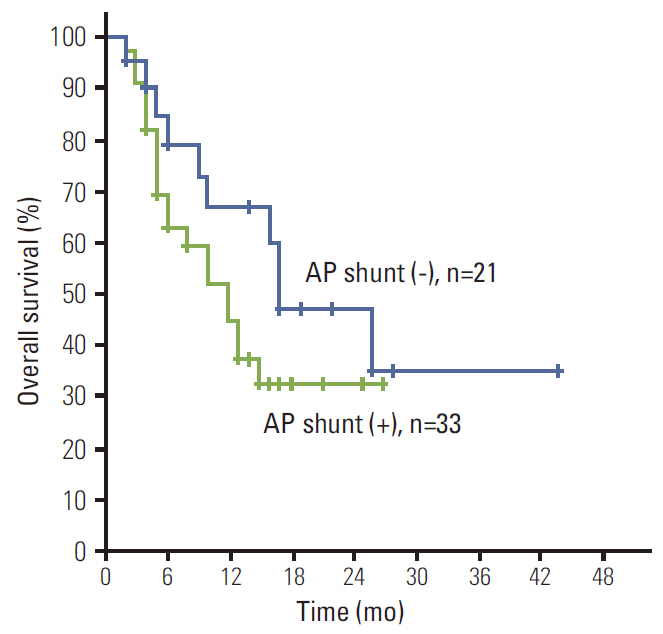
Fig. 3. The overall survival rates by presence of arterioportal (AP) shunt. The median overall survival was 17 months in patients without AP shunt and 12 months in those with AP shunt (p=0.186).
Reference
-
References
1. The Cancer of the Liver Italian Program (CLIP) Investigators. Prospective validation of the CLIP score: a new prognostic system for patients with cirrhosis and hepatocellular carcinoma. Hepatology. 2000; 31:840–5.2. Davidson BR, Gibson M, Dick R, Burroughs A, Rolles K. Incidence, risk factors, management, and outcome of portal vein abnormalities at orthotopic liver transplantation. Transplantation. 1994; 57:1174–7.
Article3. Park HC, Seong J, Tanaka M, Zeng ZC, Lim HY, Guan S, et al. Multidisciplinary management of nonresectable hepatocellular carcinoma. Oncology. 2011; 81 Suppl 1:134–40.
Article4. European Association for Study of Liver; European Organisation for Research and Treatment of Cancer. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. Eur J Cancer. 2012; 48:599–641.5. Okuda K, Musha H, Yamasaki T, Jinnouchi S, Nagasaki Y, Kubo Y, et al. Angiographic demonstration of intrahepatic arterio-portal anastomoses in hepatocellular carcinoma. Radiology. 1977; 122:53–8.
Article6. Ngan H, Peh WC. Arteriovenous shunting in hepatocellular carcinoma: its prevalence and clinical significance. Clin Radiol. 1997; 52:36–40.
Article7. Bookstein JJ, Cho KJ, Davis GB, Dail D. Arterioportal communications: observations and hypotheses concerning transsinusoidal and transvasal types. Radiology. 1982; 142:581–90.
Article8. Breen DJ, Rutherford EE, Stedman B, Lee-Elliott C, Hacking CN. Intrahepatic arterioportal shunting and anomalous venous drainage: understanding the CT features in the liver. Eur Radiol. 2004; 14:2249–60.
Article9. Huang YJ, Hsu HC, Wang CY, Wang CJ, Chen HC, Huang EY, et al. The treatment responses in cases of radiation therapy to portal vein thrombosis in advanced hepatocellular carcinoma. Int J Radiat Oncol Biol Phys. 2009; 73:1155–63.
Article10. Yoon SM, Lim YS, Won HJ, Kim JH, Kim KM, Lee HC, et al. Radiotherapy plus transarterial chemoembolization for hepatocellular carcinoma invading the portal vein: long-term patient outcomes. Int J Radiat Oncol Biol Phys. 2012; 82:2004–11.
Article11. Hsu HC, Chen TY, Chiu KW, Huang EY, Leung SW, Huang YJ, et al. Three-dimensional conformal radiotherapy for the treatment of arteriovenous shunting in patients with hepatocellular carcinoma. Br J Radiol. 2007; 80:38–42.
Article12. Yu JI, Park HC, Lim DH, Kim CJ, Oh D, Yoo BC, et al. Scheduled interval trans-catheter arterial chemoembolization followed by radiation therapy in patients with unresectable hepatocellular carcinoma. J Korean Med Sci. 2012; 27:736–43.
Article13. Oh D, Lim DH, Park HC, Paik SW, Koh KC, Lee JH, et al. Early three-dimensional conformal radiotherapy for patients with unresectable hepatocellular carcinoma after incomplete transcatheter arterial chemoembolization: a prospective evaluation of efficacy and toxicity. Am J Clin Oncol. 2010; 33:370–5.14. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010; 30:52–60.
Article15. Huang MS, Lin Q, Jiang ZB, Zhu KS, Guan SH, Li ZR, et al. Comparison of long-term effects between intra-arterially delivered ethanol and Gelfoam for the treatment of severe arterioportal shunt in patients with hepatocellular carcinoma. World J Gastroenterol. 2004; 10:825–9.
Article16. Ratti F, Cipriani F, Paganelli M, Ferla G, Aldrighetti LA. Surgical approach to multifocal hepatocellular carcinoma with portal vein thrombosis and arterioportal shunt leading to portal hypertension and bleeding: a case report. World J Surg Oncol. 2012; 10:34.
Article17. Nakai M, Sato M, Tanihata H, Sonomura T, Sahara S, Kawai N, et al. Ruptured high flow gastric varices with an intratumoral arterioportal shunt treated with balloonoccluded retrograde transvenous obliteration during temporary balloon occlusion of a hepatic artery. World J Gastroenterol. 2006; 12:5404–7.
Article18. Izaki K, Sugimoto K, Sugimura K, Hirota S. Transcatheter arterial embolization for advanced tumor thrombus with marked arterioportal or arteriovenous shunt complicating hepatocellular carcinoma. Radiat Med. 2004; 22:155–62.19. Murata S, Tajima H, Nakazawa K, Onozawa S, Kumita S, Nomura K. Initial experience of transcatheter arterial chemoembolization during portal vein occlusion for unresectable hepatocellular carcinoma with marked arterioportal shunts. Eur Radiol. 2009; 19:2016–23.
Article20. Sugano S, Miyoshi K, Suzuki T, Kawafune T, Kubota M. Intrahepatic arteriovenous shunting due to hepatocellular carcinoma and cirrhosis, and its change by transcatheter arterial embolization. Am J Gastroenterol. 1994; 89:184–8.21. Schneider BF, Eberhard DA, Steiner LE. Histopathology of arteriovenous malformations after gamma knife radiosurgery. J Neurosurg. 1997; 87:352–7.
Article22. Furuse J, Iwasaki M, Yoshino M, Konishi M, Kawano N, Kinoshita T, et al. Hepatocellular carcinoma with portal vein tumor thrombus: embolization of arterioportal shunts. Radiology. 1997; 204:787–90.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis Treated by Hepatic Artery Injection Chemotherapy and Radiotherapy
- Comparison of surgical resection versus transarterial chemoembolization with additional radiation therapy in patients with hepatocellular carcinoma with portal vein invasion
- A Case of Successful Hepatic Resection after Insufficient Response to Transarterial Chemoembolization and Radiation Therapy in Hepatocellular Carcinoma with Portal Vein Invasion
- Reappraisal of transarterial radioembolization for liver-confined hepatocellular carcinoma with portal vein tumor thrombosis: Editorial on “Transarterial radioembolization versus tyrosine kinase inhibitor in hepatocellular carcinoma with portal vein thrombosis”
- Clinical features of portal vein thrombosis in hepatocellular carcinoma
