Allergy Asthma Immunol Res.
2015 Nov;7(6):547-556. 10.4168/aair.2015.7.6.547.
Prevalence and Clinical Impact of IgE-Mediated Food Allergy in School Children With Asthma: A Double-Blind Placebo-Controlled Food Challenge Study
- Affiliations
-
- 1Department of Pediatric Allergology, Gastroenterology and Nutrition, Medical University of Lodz, Lodz, Poland. anetkrog@poczta.onet.pl
- 2Department of Pediatrics, Oncology, Hematology and Diabetes, Medical University of Lodz, Lodz, Poland.
- KMID: 2130261
- DOI: http://doi.org/10.4168/aair.2015.7.6.547
Abstract
- PURPOSE
Recent studies indirectly suggest a possible link between food allergy (FA) and asthma. Most of them have evaluated the occurrence of FA in asthmatic children, especially in the first year of life, using questionnaire-based studies or specific IgE (sIgE) assay. The aim of this study was to evaluate the prevalence and clinical impact of IgE-mediated FA in school children with asthma using a double-blind placebo-controlled food challenge (DBPCFC).
METHODS
The study group consisted of school children with atopic asthma who were admitted to the Department of Pediatric Allergology, Gastroenterology and Nutrition, Medical University of Lodz, for the evaluation of food hypersensitivity. The diagnosis of FA was established using questionnaires, sIgE analysis, and the DBPCFC. Asthma severity and asthma control state were also assessed.
RESULTS
A relationship between consumed food and complaints was reported in 180 children (49.7%). Seventy children (19.3%) were sensitized to food allergens. IgE-mediated FA was confirmed in 24 children (6.6%), while 11 children (3%) demonstrated respiratory symptoms. Food-induced asthma exacerbations were observed in 9 patients (2.5%). Statistically significant differences in the prevalence of atopic dermatitis (P<0.002), urticaria (P<0.03), digestive symptoms (P<0.03), rhinitis (P<0.02), sIgE level (P<0.001), positive family history of atopy (P<0.001) and FA in history (P<0.001) were found between asthmatic children with FA and those without. Children with food-induced asthma exacerbations demonstrated significantly greater severity, poorer controls, and worse morbidity compared to those without.
CONCLUSIONS
Although food-induced respiratory reactions in children with asthma were rare, they were classified as severe and associated with worse morbidity, greater severity, and poorer control. As the most commonly observed symptoms were coughing and rhinitis, which can be easily misdiagnosed, a proper diagnosis is essential for improving the management of both clinical conditions.
MeSH Terms
Figure
-
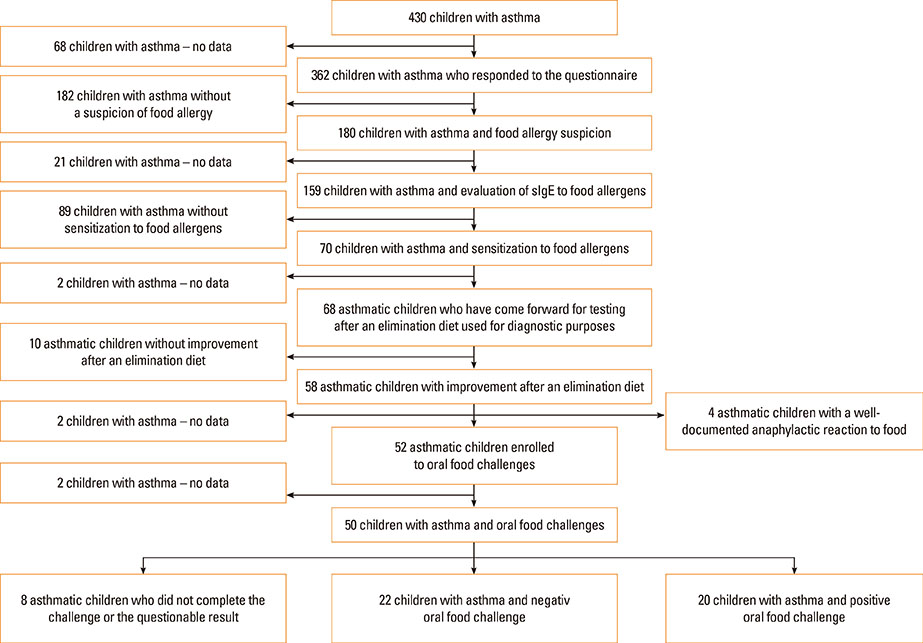
Fig. 1 Study design. Flow chart depicting steps involved in patient selection and tests in this study.
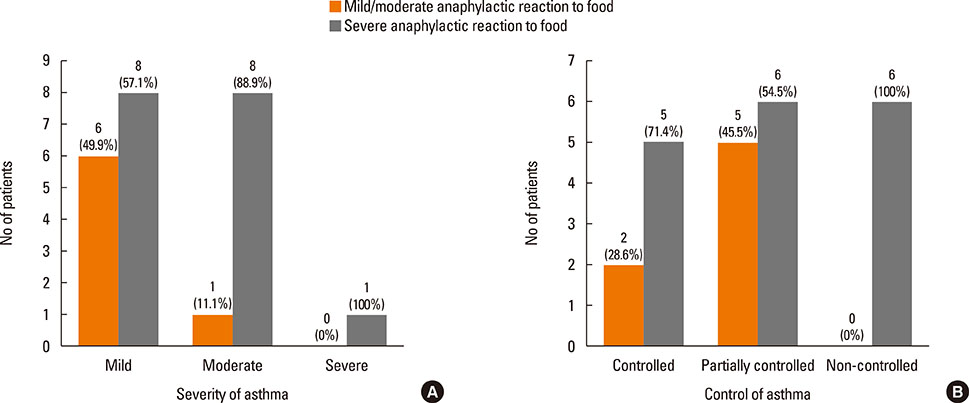
Fig. 2 Degrees of asthma severity (A) and control (B) in association with the degree of food reactions after the OFC in children with asthma and food allergy.
Cited by 1 articles
-
Accurate Determination of Childhood Food Allergy Prevalence and Correction of Unnecessary Avoidance
Yuki Okada, Takumi Yamashita, Hideki Kumagai, Yoshihiko Morikawa, Akira Akasawa
Allergy Asthma Immunol Res. 2017;9(4):322-328. doi: 10.4168/aair.2017.9.4.322.
Reference
-
1. Roberts G, Lack G. Food allergy and asthma--what is the link? Paediatr Respir Rev. 2003; 4:205–212.2. Kewalramani A, Bollinger ME. The impact of food allergy on asthma. J Asthma Allergy. 2010; 3:65–74.3. Beausoleil JL, Fiedler J, Spergel JM. Food intolerance and childhood asthma: what is the link? Paediatr Drugs. 2007; 9:157–163.4. Pénard-Morand C, Raherison C, Kopferschmitt C, Caillaud D, Lavaud F, Charpin D, et al. Prevalence of food allergy and its relationship to asthma and allergic rhinitis in schoolchildren. Allergy. 2005; 60:1165–1171.5. Schroeder A, Kumar R, Pongracic JA, Sullivan CL, Caruso DM, Costello J, et al. Food allergy is associated with an increased risk of asthma. Clin Exp Allergy. 2009; 39:261–270.6. Zheng T, Yu J, Oh MH, Zhu Z. The atopic march: progression from atopic dermatitis to allergic rhinitis and asthma. Allergy Asthma Immunol Res. 2011; 3:67–73.7. Pyun BY. Natural history and risk factors of atopic dermatitis in children. Allergy Asthma Immunol Res. 2015; 7:101–105.8. Jaramillo R, Massing M, Sicherer SH, Wood RA, Bock SA, Burks AW, et al. High-level sensitization to foods is associated with asthma ER visits and current asthma in the U.S.: results from NHANES 2005-2006. J Allergy Clin Immunol. 2009; 123:S111.9. Cuesta-Herranz J, Barber D, Blanco C, Cistero-Bahíma A, Crespo JF, Fernández-Rivas M, et al. Differences among pollen-allergic patients with and without plant food allergy. Int Arch Allergy Immunol. 2010; 153:182–192.10. Wang J, Visness CM, Sampson HA. Food allergen sensitization in inner-city children with asthma. J Allergy Clin Immunol. 2005; 115:1076–1080.11. Woods RK, Weiner J, Abramson M, Thien F, Walters EH. Patients' perceptions of food-induced asthma. Aust N Z J Med. 1996; 26:504–512.12. Park M, Kim D, Ahn K, Kim J, Han Y. Prevalence of immediate-type food allergy in early childhood in Seoul. Allergy Asthma Immunol Res. 2014; 6:131–136.13. Bock SA. Respiratory reactions induced by food challenges in children with pulmonary disease. Pediatr Allergy Immunol. 1992; 3:188–194.14. Simpson AB, Yousef E, Hossain J. Association between peanut allergy and asthma morbidity. J Pediatr. 2010; 156:777–781. 781.e115. Simpson AB, Glutting J, Yousef E. Food allergy and asthma morbidity in children. Pediatr Pulmonol. 2007; 42:489–495.16. Liu AH, Jaramillo R, Sicherer SH, Wood RA, Bock SA, Burks AW, et al. National prevalence and risk factors for food allergy and relationship to asthma: results from the National Health and Nutrition Examination Survey 2005-2006. J Allergy Clin Immunol. 2010; 126:798–806.e13.17. Roberts G, Patel N, Levi-Schaffer F, Habibi P, Lack G. Food allergy as a risk factor for life-threatening asthma in childhood: a case-controlled study. J Allergy Clin Immunol. 2003; 112:168–174.18. Gillman A, Douglass JA. What do asthmatics have to fear from food and additive allergy? Clin Exp Allergy. 2010; 40:1295–1302.19. Vogel NM, Katz HT, Lopez R, Lang DM. Food allergy is associated with potentially fatal childhood asthma. J Asthma. 2008; 45:862–866.20. Patelis A, Janson C, Borres MP, Nordvall L, Alving K, Malinovschi A. Aeroallergen and food IgE sensitization and local and systemic inflammation in asthma. Allergy. 2014; 69:380–387.21. Baena-Cagnani CE, Teijeiro A. Role of food allergy in asthma in childhood. Curr Opin Allergy Clin Immunol. 2001; 1:145–149.22. Quirce S, Diaz-Perales A. Diagnosis and management of grain-induced asthma. Allergy Asthma Immunol Res. 2013; 5:348–356.23. James JM. Respiratory manifestations of food allergy. Pediatrics. 2003; 111:1625–1630.24. Bousquet J, Neukirch F, Noyola A, Michel FB. Prevalence of food allergy in asthma. Pediatr Allergy Immunol. 1992; 3:206–213.25. National Institutes of Health. National Heart, Lung, and Blood Institute (US). Global strategy for asthma management and prevention NIH Publication No 02-3659 [Internet]. [place unknown]s: Global Initiative for Asthma;2002. cited 2015 Mar 26. Available from: http://www.ginasthma.org/local/uploads/files/GINAwr02.pdf.26. Liu AH, Zeiger R, Sorkness C, Mahr T, Ostrom N, Burgess S, et al. Development and cross-sectional validation of the Childhood Asthma Control Test. J Allergy Clin Immunol. 2007; 119:817–825.27. Park SY, Yoon SY, Shin B, Kwon HS, Kim TB, Moon HB, et al. Clinical factors affecting discrepant correlation between asthma control test score and pulmonary function. Allergy Asthma Immunol Res. 2015; 7:83–87.28. Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005; 26:948–968.29. Bindslev-Jensen C, Ballmer-Weber BK, Bengtsson U, Blanco C, Ebner C, Hourihane J, et al. Standardization of food challenges in patients with immediate reactions to foods--position paper from the European Academy of Allergology and Clinical Immunology. Allergy. 2004; 59:690–697.30. Nowak-Wegrzyn A, Assa'ad AH, Bahna SL, Bock SA, Sicherer SH, Teuber SS, et al. Work Group report: oral food challenge testing. J Allergy Clin Immunol. 2009; 123:S365–S383.31. Sampson HA. Anaphylaxis and emergency treatment. Pediatrics. 2003; 111:1601–1608.32. Benhamou AH, Zamora SA, Eigenmann PA. Correlation between specific immunoglobulin E levels and the severity of reactions in egg allergic patients. Pediatr Allergy Immunol. 2008; 19:173–179.33. Novembre E, de Martino M, Vierucci A. Foods and respiratory allergy. J Allergy Clin Immunol. 1988; 81:1059–1065.34. Rancé F, Dutau G. Asthma and food allergy: report of 163 pediatric cases. Arch Pediatr. 2002; 9:Suppl 3. 402s–407s.35. Roehr CC, Edenharter G, Reimann S, Ehlers I, Worm M, Zuberbier T, et al. Food allergy and non-allergic food hypersensitivity in children and adolescents. Clin Exp Allergy. 2004; 34:1534–1541.36. Caffarelli C, Deriu FM, Terzi V, Perrone F, De Angelis G, Atherton DJ. Gastrointestinal symptoms in patients with asthma. Arch Dis Child. 2000; 82:131–135.37. Kumar R, Kumari D, Srivastava P, Khare V, Fakhr H, Arora N, et al. Identification of IgE-mediated food allergy and allergens in older children and adults with asthma and allergic rhinitis. Indian J Chest Dis Allied Sci. 2010; 52:217–224.38. Calamelli E, Ricci G, Dell'Omo V, Bendandi B, Masi M. Food allergy in children with asthma: prevalence and correlation with clinical severity of respiratory disease. Open Allergy J. 2015; 1:5–11.39. Rona RJ, Keil T, Summers C, Gislason D, Zuidmeer L, Sodergren E, et al. The prevalence of food allergy: a meta-analysis. J Allergy Clin Immunol. 2007; 120:638–646.40. Zuidmeer L, Goldhahn K, Rona RJ, Gislason D, Madsen C, Summers C, et al. T he prevalence of plant food allergies: a systematic review. J Allergy Clin Immunol. 2008; 121:1210–1218.e4.41. Bedolla-Barajas M, Bedolla-Pulido TR, Camacho-Peña AS, González-García E, Morales-Romero J. Food hypersensitivity in mexican adults at 18 to 50 years of age: a questionnaire survey. Allergy Asthma Immunol Res. 2014; 6:511–516.42. James JM, Bernhisel-Broadbent J, Sampson HA. Respiratory reactions provoked by double-blind food challenges in children. Am J Respir Crit Care Med. 1994; 149:59–64.43. Bock SA, Muñoz-Furlong A, Sampson HA. Further fatalities caused by anaphylactic reactions to food, 2001-2006. J Allergy Clin Immunol. 2007; 119:1016–1018.44. Roberts G. Anaphylaxis to foods. Pediatr Allergy Immunol. 2007; 18:543–548.45. Graif Y, German L, Livne I, Shohat T. Association of food allergy with asthma severity and atopic diseases in Jewish and Arab adolescents. Acta Paediatr. 2012; 101:1083–1088.46. Friedlander JL, Sheehan WJ, Baxi SN, Kopel LS, Gaffin JM, Ozonoff A, et al. Food allergy and increased asthma morbidity in a School-based Inner-City Asthma Study. J Allergy Clin Immunol Pract. 2013; 1:479–484.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Food Allergy: Diagnosis and Management
- The Diagnosis of Food Allergy in a Pediatric Gastroenterology: Focusing on Non-IgE-mediated Allergic Diseases
- Diagnosis and Treatment of Food Allergy in Children
- Clinical Perspectives of Food Allergy in Infants and Young Children
- Characterization of food allergies in patients with atopic dermatitis
