J Gynecol Oncol.
2014 Jul;25(3):206-213. 10.3802/jgo.2014.25.3.206.
Ultrasound guided conformal brachytherapy of cervix cancer: survival, patterns of failure, and late complications
- Affiliations
-
- 1Peter MacCallum Cancer Centre and University of Melbourne, East Melbourne, VIC, Australia. mahaguru@petermac.org
- 2Radiation Therapy Services, Peter MacCallum Cancer Centre, East Melbourne, VIC, Australia.
- 3Division of Radiation Oncology, Peter MacCallum Cancer Centre, East Melbourne, VIC, Australia.
- 4Division of Medical Oncology, Peter MacCallum Cancer Centre, East Melbourne, VIC, Australia.
- 5Rural Clinical School, The University of Queensland School of Medicine, Toowoomba, QLD, Australia.
- KMID: 2130101
- DOI: http://doi.org/10.3802/jgo.2014.25.3.206
Abstract
OBJECTIVE
The aim of this study was to report on the long-term results of transabdominal ultrasound guided conformal brachytherapy in patients with cervical cancer with respect to patterns of failures, treatment related toxicities and survival.
METHODS
Three hundred and nine patients with cervical cancer who presented to Institute between January 1999 and December 2008 were staged with magnetic resonance imaging and positron emission tomography and treated with external beam radiotherapy and high dose rate conformal image guided brachytherapy with curative intent. Follow-up data relating to sites of failure and toxicity was recorded prospectively.
RESULTS
Two hundred and ninety-two patients were available for analyses. The median (interquantile range) follow-up time was 4.1 years (range, 2.4 to 6.1 years). Five-year failure free survival and overall survival (OS) were 66% and 65%, respectively. Primary, pelvic, para-aortic, and distant failure were observed in 12.5%, 16.4%, 22%, and 23% of patients, respectively. In multivariate analysis, tumor volume and nodal disease related to survival, whereas local disease control and point A dose did not.
CONCLUSION
Ultrasound guided conformal brachytherapy of cervix cancer has led to optimal local control and OS. The Melbourne protocol compares favorably to the more technically elaborate and expensive GEC-ESTRO recommendations. The Melbourne protocol's technical simplicity with real-time imaging and treatment planning makes this a method of choice for treating patients with cervical cancer.
MeSH Terms
-
Adenocarcinoma/pathology/radiography/secondary/ultrasonography
Adult
Aged
Brachytherapy/adverse effects/*methods
Carcinoma, Squamous Cell/pathology/radiography/secondary/ultrasonography
Female
Follow-Up Studies
Humans
Kaplan-Meier Estimate
Lymphatic Metastasis
Middle Aged
Neoplasm Staging
Prognosis
Prospective Studies
Radiation Dosage
Radiotherapy, Conformal/adverse effects/*methods
Treatment Failure
Ultrasonography, Interventional/*methods
Uterine Cervical Neoplasms/pathology/*radiography/ultrasonography
Figure
-
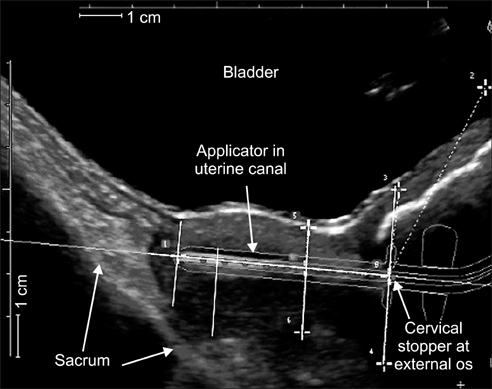
Fig. 1 Sagittal ultrasound view of uterus and cervix with treatment applicator in situ. Organ dimensions are obtained by measuring the distance from the applicator to the uterine cervix surface at 2.0 cm intervals along the applicator from the cervical stopper to the tip of the applicator. Source: Peter MacCallum Cancer Centre [6,8].
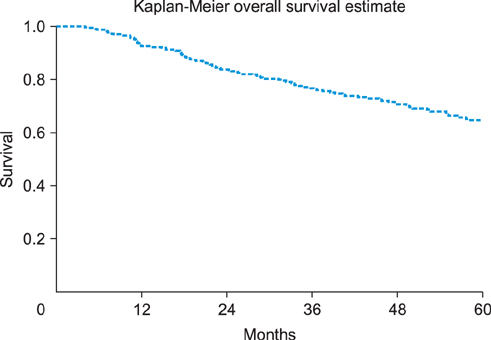
Fig. 2 Overall survival.
Reference
-
1. Narayan K, McKenzie A, Fisher R, Susil B, Jobling T, Bernshaw D. Estimation of tumor volume in cervical cancer by magnetic resonance imaging. Am J Clin Oncol. 2003; 26:e163–e168.2. International Commission on Radiological Units and Measurements. Dose and volume specification for reporting intracavitary therapy in gynecology. Bethesda: International Commission on Radiological Units and Measurements, Inc;1985.3. Narayan K, van Dyk S, Bernshaw D, Rajasooriyar C, Kondalsamy-Chennakesavan S. Comparative study of LDR (Manchester system) and HDR image-guided conformal brachytherapy of cervical cancer: patterns of failure, late complications, and survival. Int J Radiat Oncol Biol Phys. 2009; 74:1529–1535.4. Narayan K, Fisher R, Bernshaw D. Significance of tumor volume and corpus uteri invasion in cervical cancer patients treated by radiotherapy. Int J Gynecol Cancer. 2006; 16:623–630.5. Narayan K, Fisher RJ, Bernshaw D. Patterns of failure and prognostic factor analyses in locally advanced cervical cancer patients staged by magnetic resonance imaging and treated with curative intent. Int J Gynecol Cancer. 2008; 18:525–533.6. Van Dyk S, Narayan K, Fisher R, Bernshaw D. Conformal brachytherapy planning for cervical cancer using transabdominal ultrasound. Int J Radiat Oncol Biol Phys. 2009; 75:64–70.7. Nag S, Gupta N. A simple method of obtaining equivalent doses for use in HDR brachytherapy. Int J Radiat Oncol Biol Phys. 2000; 46:507–513.8. van Dyk S, Kondalsamy-Chennakesavan S, Schneider M, Bernshaw D, Narayan K. Comparison of measurements of the uterus and cervix obtained by magnetic resonance and transabdominal ultrasound imaging to identify the brachytherapy target in patients with cervix cancer. Int J Radiat Oncol Biol Phys. 2014; 88:860–865.9. Suit HD, Westgate SJ. Impact of improved local control on survival. Int J Radiat Oncol Biol Phys. 1986; 12:453–458.10. Barkati M, Van Dyk S, Foroudi F, Narayan K. The use of magnetic resonance imaging for image-guided brachytherapy. J Med Imaging Radiat Oncol. 2010; 54:137–141.11. Potter R, Dimopoulos J, Georg P, Lang S, Waldhausl C, Wachter-Gerstner N, et al. Clinical impact of MRI assisted dose volume adaptation and dose escalation in brachytherapy of locally advanced cervix cancer. Radiother Oncol. 2007; 83:148–155.12. Mackie TR, Kapatoes J, Ruchala K, Lu W, Wu C, Olivera G, et al. Image guidance for precise conformal radiotherapy. Int J Radiat Oncol Biol Phys. 2003; 56:89–105.13. Narayan K, McKenzie AF, Hicks RJ, Fisher R, Bernshaw D, Bau S. Relation between FIGO stage, primary tumor volume, and presence of lymph node metastases in cervical cancer patients referred for radiotherapy. Int J Gynecol Cancer. 2003; 13:657–663.14. Narayan K, Fisher RJ, Bernshaw D, Shakher R, Hicks RJ. Patterns of failure and prognostic factor analyses in locally advanced cervical cancer patients staged by positron emission tomography and treated with curative intent. Int J Gynecol Cancer. 2009; 19:912–918.15. Haie-Meder C, Chargari C, Rey A, Dumas I, Morice P, Magne N. MRI-based low dose-rate brachytherapy experience in locally advanced cervical cancer patients initially treated by concomitant chemoradiotherapy. Radiother Oncol. 2010; 96:161–165.16. Potter R, Georg P, Dimopoulos JC, Grimm M, Berger D, Nesvacil N, et al. Clinical outcome of protocol based image (MRI) guided adaptive brachytherapy combined with 3D conformal radiotherapy with or without chemotherapy in patients with locally advanced cervical cancer. Radiother Oncol. 2011; 100:116–123.17. Lindegaard JC, Fokdal LU, Nielsen SK, Juul-Christensen J, Tanderup K. MRI-guided adaptive radiotherapy in locally advanced cervical cancer from a Nordic perspective. Acta Oncol. 2013; 52:1510–1519.18. Dimopoulos JC, Petrow P, Tanderup K, Petric P, Berger D, Kirisits C, et al. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (IV): basic principles and parameters for MR imaging within the frame of image based adaptive cervix cancer brachytherapy. Radiother Oncol. 2012; 103:113–122.19. Narayan K, Barkati M, van Dyk S, Bernshaw D. Image-guided brachytherapy for cervix cancer: from Manchester to Melbourne. Expert Rev Anticancer Ther. 2010; 10:41–46.20. Rajasooriyar C, Van Dyk S, Lindawati M, Bernshaw D, Kondalsamy-Chennakesavan S, Narayan K. Reviewing the role of parametrial boost in patients with cervical cancer with clinically involved parametria and staged with positron emission tomography. Int J Gynecol Cancer. 2012; 22:1532–1537.21. Schmid MP, Fidarova E, Potter R, Petric P, Bauer V, Woehs V, et al. Magnetic resonance imaging for assessment of parametrial tumour spread and regression patterns in adaptive cervix cancer radiotherapy. Acta Oncol. 2013; 52:1384–1390.22. Delpech Y, Haie-Meder C, Rey A, Zafrani Y, Uzan C, Gouy S, et al. Para-aortic involvement and interest of para-aortic lymphadenectomy after chemoradiation therapy in patients with stage IB2 and II cervical carcinoma radiologically confined to the pelvic cavity. Ann Surg Oncol. 2007; 14:3223–3231.23. Morice P, Castaigne D, Pautier P, Rey A, Haie-Meder C, Leblanc M, et al. Interest of pelvic and paraaortic lymphadenectomy in patients with stage IB and II cervical carcinoma. Gynecol Oncol. 1999; 73:106–110.24. Touboul C, Uzan C, Mauguen A, Gouy S, Rey A, Pautier P, et al. Prognostic factors and morbidities after completion surgery in patients undergoing initial chemoradiation therapy for locally advanced cervical cancer. Oncologist. 2010; 15:405–415.25. Narayan K, vanDyk S, Bernshaw DL. In regard to correspondence between Potter et al. and Nag et al. (Int J Radiat Oncol Biol Phys 2005;62:293-295). Int J Radiat Oncol Biol Phys. 2005; 63:644–645.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Radiotherapy Results of Early Uterine Cervix Cancer
- Radiation Treatment for Prostate Cancer
- Radiation therapy of cervical cancer: Current status in Korea and recent developments
- Use of transrectal ultrasound for high dose rate interstitial brachytherapy for patients of carcinoma of uterine cervix
- High Versus Low Dose-Rate Intracavitary Irradiation for Adenocarcinoma of the Uterine Cervix
