Association between Bone Mineral Density and Clinical Consequences: Cross-Sectional Study of Korean Postmenopausal Women in an Orthopaedic Outpatient Clinic
- Affiliations
-
- 1Department of Orthopaedic Surgery, College of Medicine, Seoul National University, Seoul, Korea. spinelee@snu.ac.kr
- 2Department of Orthopaedic Surgery, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul, Korea.
- 3Department of Orthopaedic Surgery, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2129613
- DOI: http://doi.org/10.3346/jkms.2014.29.8.1152
Abstract
- This study is to identify the characteristics of BMD and the related clinical consequences through a nationwide, consecutive, cross-sectional study. A total of 1,281 postmenopausal women was enrolled nationwide and underwent measurement for BMD using dual energy x-ray absorptiometry. Following the T-spine and L-spine plane radiography, they were evaluated for vertebral fracture by a semi-quantitative method using the Genant's method. Relationship between BMD and osteoporotic fracture and a degree of deformity in vertebral fracture, treatment history in osteoporosis and the EQ-5D was analyzed. The distribution of the normal, osteopenia and osteoporosis group was 25.9%, 37.0%, and 37.2% in lumbar spine, and 31.4%, 45.3%, and 23.3% in femur neck, respectively. BMD in subjects with symptomatic or asymptomatic vertebral fracture was significantly lower than those without fracture. The femur neck and total hip BMDs were significantly lower in hip fracture group (0.646 g/cm2 and 0.643 g/cm2, respectively) and wrist fracture group (0.661 g/cm2 and 0.712 g/cm2, respectively) than in subjects without fracture (0.721 g/cm2 and 0.712 g/cm2, respectively). The BMD was significantly lower with more severe degree of deformity in vertebral fracture and lower scores in mobility, usual activities and pain/discomfort of the EQ-5D. In Korean postmenopausal women, the prevalence of osteoporosis and vertebral, hip and wrist fracture increase and quality of life decreases with lower BMD.
Keyword
MeSH Terms
-
Aged
Aged, 80 and over
*Bone Density
Comorbidity
Cross-Sectional Studies
Female
Humans
Incidence
Middle Aged
Osteoporosis, Postmenopausal/*epidemiology/*radiography
Osteoporotic Fractures/*epidemiology/*radiography
Postmenopause
Reproducibility of Results
Republic of Korea/epidemiology
Risk Assessment
Sensitivity and Specificity
Statistics as Topic
Women's Health/statistics & numerical data
Figure
-
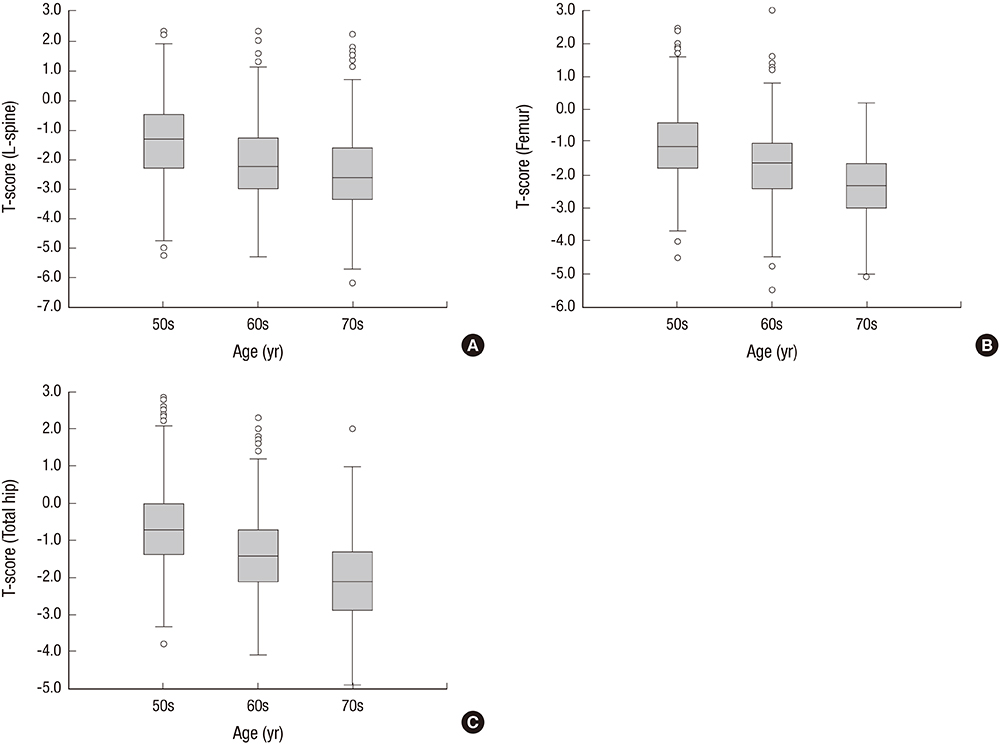
Fig. 1 T-scores by age group: Box plot. (A) T-score of L-spine. (B) T-score of femur neck. (C) T-score of total hip. With increasing age, the L-spine, femur neck and total hip BMD values significantly decrease.
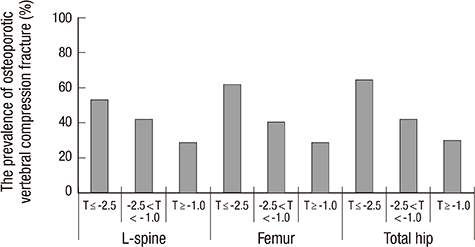
Fig. 2 The incidence of osteoporotic vertebral compression fracture by T-score. With decreasing T-score, the prevalence of vertebral compression fracture increase.
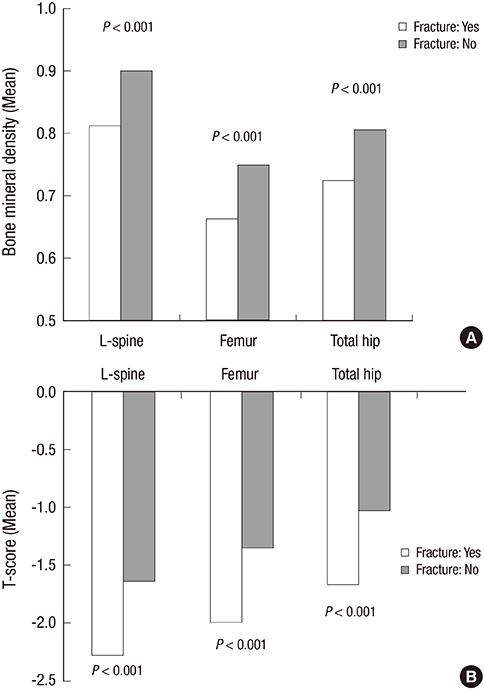
Fig. 3 Bone mineral density and fracture. (A) The mean BMD values in the L-spine, femur neck and total hip was significantly lower in subjects with osteoporotic vertebral fracture than those without fracture (P < 0.001 for all three). (B) T-scores in the L-spine, femur neck and total hip was also significantly lower in subjects with osteoporotic vertebral fracture than those without fracture (P < 0.001 for all three).
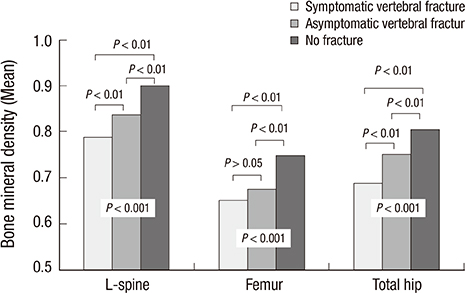
Fig. 4 Bone mineral density and osteoporotic vertebral compression fracture with or without pain. The L-spine and total hip BMD values was significantly lower in vertebral fracture patients with pain than in asymptomatic fracture patients (P < 0.01 for all), and BMD values in the L-spine, femur neck and total hip was significantly lower in asymptomatic fracture patients than those without vertebral fracture (P < 0.01 for all) by analysis of variance.
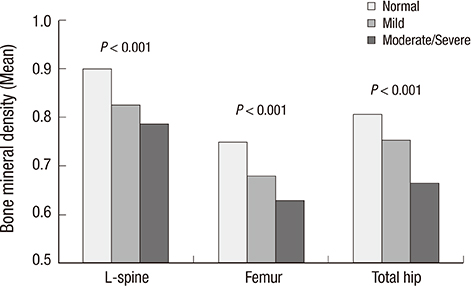
Fig. 5 Bone mineral density by vertebral deformity grade. The L-spine, femur neck and total hip BMD are significantly higher in the normal group than that in the Genant SQ Grade 1 and the Genant SQ Grade 2 and 3 group (P < 0.01). The femur neck and total hip BMD are significantly higher in Genant SQ Grade 1 than the Genant SQ Grade 2 and 3 (P < 0.01) by analysis of variance (ANOVA).

Fig. 6 Correlation between the EQ-5D index and VAS. The EQ-5D index shows a weak correlation coefficient of r = 0.445 with VAS (P < 0.001).
Cited by 2 articles
-
Health-related Quality of Life in Accordance with Fracture History and Comorbidities in Korean Patients with Osteoporosis
Hye-Young Kwon, Yong-Chan Ha, Jun-Il Yoo
J Bone Metab. 2016;23(4):199-206. doi: 10.11005/jbm.2016.23.4.199.Cost-effectiveness of Pharmaceutical Interventions to Prevent Osteoporotic Fractures in Postmenopausal Women with Osteopenia
Jin-Won Kwon, Hae-Young Park, Ye Jee Kim, Seong-Hwan Moon, Hye-Young Kang
J Bone Metab. 2016;23(2):63-77. doi: 10.11005/jbm.2016.23.2.63.
Reference
-
1. Suzuki T, Yoshida H. Low bone mineral density at femoral neck is a predictor of increased mortality in elderly Japanese women. Osteoporos Int. 2010; 21:71–79.2. Cauley JA. Defining ethnic and racial differences in osteoporosis and fragility fractures. Clin Orthop Relat Res. 2011; 469:1891–1899.3. Kanis JA, Burlet N, Cooper C, Delmas PD, Reginster JY, Borgstrom F, Rizzoli R. European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int. 2008; 19:399–428.4. Kanis JA, Johnell O, De Laet C, Jonsson B, Oden A, Ogelsby AK. International variations in hip fracture probabilities: implications for risk assessment. J Bone Miner Res. 2002; 17:1237–1244.5. Yoon HK, Park C, Jang S, Jang S, Lee YK, Ha YC. Incidence and mortality following hip fracture in Korea. J Korean Med Sci. 2011; 26:1087–1092.6. Haleem S, Lutchman L, Mayahi R, Grice JE, Parker MJ. Mortality following hip fracture: trends and geographical variations over the last 40 years. Injury. 2008; 39:1157–1163.7. Lau E, Ong K, Kurtz S, Schmier J, Edidin A. Mortality following the diagnosis of a vertebral compression fracture in the Medicare population. J Bone Joint Surg Am. 2008; 90:1479–1486.8. Puisto V, Rissanen H, Heliövaara M, Impivaara O, Jalanko T, Kröger H, Knekt P, Aromaa A, Helenius I. Vertebral fracture and cause-specific mortality: a prospective population study of 3,210 men and 3,730 women with 30 years of follow-up. Eur Spine J. 2011; 20:2181–2186.9. Lee YK, Jang S, Jang S, Lee HJ, Park C, Ha YC, Kim DY. Mortality after vertebral fracture in Korea: analysis of the National Claim Registry. Osteoporos Int. 2012; 23:1859–1865.10. Fujiwara S, Kasagi F, Masunari N, Naito K, Suzuki G, Fukunaga M. Fracture prediction from bone mineral density in Japanese men and women. J Bone Miner Res. 2003; 18:1547–1553.11. Kim DH, Vaccaro AR. Osteoporotic compression fractures of the spine; current options and considerations for treatment. Spine J. 2006; 6:479–487.12. Genant HK, Wu CY, van Kuijk C, Nevitt MC. Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res. 1993; 8:1137–1148.13. Lee YK, Nam HS, Chuang LH, Kim KY, Yang HK, Kwon IS, Kind P, Kweon SS, Kim YT. South Korean time trade-off values for EQ-5D health states: modeling with observed values for 101 health states. Value Health. 2009; 12:1187–1193.14. Albala C, Yáñez M, Devoto E, Sostin C, Zeballos L, Santos JL. Obesity as a protective factor for postmenopausal osteoporosis. Int J Obes Relat Metab Disord. 1996; 20:1027–1032.15. Reid IR, Plank LD, Evans MC. Fat mass is an important determinant of whole body bone density in premenopausal women but not in men. J Clin Endocrinol Metab. 1992; 75:779–782.16. Zhao LJ, Jiang H, Papasian CJ, Maulik D, Drees B, Hamilton J, Deng HW. Correlation of obesity and osteoporosis: effect of fat mass on the determination of osteoporosis. J Bone Miner Res. 2008; 23:17–29.17. Greco EA, Fornari R, Rossi F, Santiemma V, Prossomariti G, Annoscia C, Aversa A, Brama M, Marini M, Donini LM, et al. Is obesity protective for osteoporosis? Evaluation of bone mineral density in individuals with high body mass index. Int J Clin Pract. 2010; 64:817–820.18. Kim KC, Shin DH, Lee SY, Im JA, Lee DC. Relation between obesity and bone mineral density and vertebral fractures in Korean postmenopausal women. Yonsei Med J. 2010; 51:857–863.19. Mussolino ME, Madans JH, Gillum RF. Bone mineral density and mortality in women and men: the NHANES I epidemiologic follow-up study. Ann Epidemiol. 2003; 13:692–697.20. Yu W, Glüer CC, Fuerst T, Grampp S, Li J, Lu Y, Genant HK. Influence of degenerative joint disease on spinal bone mineral measurements in postmenopausal women. Calcif Tissue Int. 1995; 57:169–174.21. Black DM, Cummings SR, Stone K, Hudes E, Palermo L, Steiger P. A new approach to defining normal vertebral dimensions. J Bone Miner Res. 1991; 6:883–892.22. Kanis JA. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: synopsis of a WHO report: WHO Study Group. Osteoporos Int. 1994; 4:368–381.23. Lindsey C, Brownbill RA, Bohannon RA, Ilich JZ. Association of physical performance measures with bone mineral density in postmenopausal women. Arch Phys Med Rehabil. 2005; 86:1102–1107.24. Yoh K, Tanaka K, Ishikawa A, Ishibashi T, Uchino Y, Sato Y, Tobinaga M, Hasegawa N, Kamae S, Yoshizawa M. Health-related quality of life (HRQOL) in Japanese osteoporotic patients and its improvement by elcatonin treatment. J Bone Miner Metab. 2005; 23:167–173.25. Sim IW, Ebeling PR. Treatment of osteoporosis in men with bisphosphonates: rationale and latest evidence. Ther Adv Musculoskelet Dis. 2013; 5:259–267.26. Lee JH, Lee YH, Moon SH, Lee YS. Prevalence of Osteoporotic Vertebral Compression Fractures in Korean Post Menopausal Women Study Group. Influence of insurance benefit criteria on the administration rate of osteoporosis drugs in postmenopausal females. Clin Orthop Surg. 2014; 6:56–61.27. Fu X, Zhao X, Lu H, Jiang F, Ma X, Zhu S. Association between sleep duration and bone mineral density in Chinese women. Bone. 2011; 49:1062–1066.28. Coelho R, Silva C, Maia A, Prata J, Barros H. Bone mineral density and depression: a community study in women. J Psychosom Res. 1999; 46:29–35.29. Lekamwasam S, Trivedi DP, Khaw KT. An association between respiratory function and bone mineral density in women from the general community: a cross sectional study. Osteoporos Int. 2002; 13:710–715.30. Laudisio A, Marzetti E, Antonica L, Cocchi A, Bernabei R, Zuccalà G. Association of left ventricular function with bone mineral density in older women: a population-based study. Calcif Tissue Int. 2008; 82:27–33.31. Tankó LB, Christiansen C, Cox DA, Geiger MJ, McNabb MA, Cummings SR. Relationship between osteoporosis and cardiovascular disease in postmenopausal women. J Bone Miner Res. 2005; 20:1912–1920.32. Van Der Klift M, Pols HA, Geleijnse JM, Van Der Kuip DA, Hofman A, De Laet CE. Bone mineral density and mortality in elderly men and women: the Rotterdam Study. Bone. 2002; 30:643–648.33. Browner WS, Seeley DG, Vogt TM, Cummings SR. Non-trauma mortality in elderly women with low bone mineral density: Study of Osteoporotic Fractures Research Group. Lancet. 1991; 338:355–358.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The relationship of maturation value of vaginal epithelium and bone mineral density in postmenopausal women
- Change in bone mineral density according to aging in Korean women: Study of Using Quantitative Computerized Tomography
- Investigation of Comorbidity, Trauma History, and Osteoporotic Fractures in the Postmenopausal Population: A Nationwide, Observational, and Cross-Sectional Study of Korean Orthopedic Outpatient Clinics
- The Relationship of Subclinical Hypothyroidism with Bone Mineral Density and Biochemical Bone Markers in Postmenopausal Women
- High Serum Osteopontin Levels Are Associated with Low Bone Mineral Density in Postmenopausal Women
