Cancer Res Treat.
2004 Apr;36(2):157-159.
Isolated Diaphragmatic Metastasis Originated from Adenocarcinoma of the Colon
- Affiliations
-
- 1Colorectal Clinic, Department of Surgery, University of Ulsan College of Medicine and Asan Medical Center, Seoul, Korea. csyu@amc.seoul.kr
- 2Department of Surgery, University of Dankook College of Medicine, Cheonan, Korea.
Abstract
- Isolated diaphragmatic metastasis arising from colorectal cancer has been reported only one case in the literature presently. Here, we presented a new case and discussed the possible pathogenesis and the treatment options. A 42-year-old male patient had received anterior resection for sigmoid colon cancer. Although the increased serum CEA level was detected 20 months after the surgery, metastatic lesion could not be detected by repeated colonoscopy, CT scan, bone scan or PET scan for 35 months. We could detect a suspicious metastatic lesion on the liver by CT scan at 56 month after the surgery. During a second-look operation, we found a solitary metastasis on the diaphragm and removed it along with the 1 cm tumor-free resection margin. Although the prognosis associated with skeletal metastasis is poor, the complete resection of isolated diaphragmatic metastasis and subsequent appropriate adjuvant chemotherapy may achieve a cure the disease provided that other metastatic lesions are absent.
MeSH Terms
Figure
-
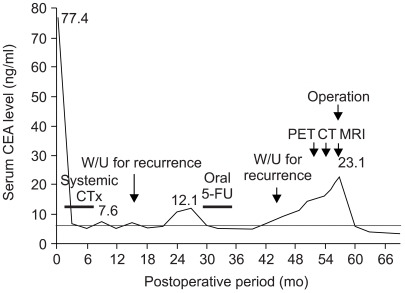
Fig. 1 Clinical course of the patient: the close correlation between serum CEA level and treatment response.

Fig. 2 MRI of an isolated metastatic tumor on the diaphragm. (A) Gadolinium enhanced T1-weighted axial view showed a ill-defined peripherally enhanced low signal lesion (arrow). (B) coronal view showed a protruding mass with motion artifact (arrow).

Fig. 3 Histopathological findings. (A) primary sigmoid colon cancer (H&E, ×200). (B-C) isolated metastasis on the diaphragm. The metastatic tumor, which involved entire thickness of the diaphragm, had a moderate cellular differentiation and amount of mucin similar to that of the primary sigmoid colon cancer (H&E, ×200, ×40).
Reference
-
1. Devesa JM, Morales V, Enriquez JM. Colorectal cancer. The bases for a comprehensive follow-up. Dis Colon Rectum. 1988; 31:636–652. PMID: 3042304.2. Brennan JL. Metastatic tumors of the diaphragm. Br J Surg. 1971; 58:458–460. PMID: 4932851.3. Funatsu K, Nishihara H, Nozaki Y, Sakai T, Tomoda N, Itoh Y, Hayabuchi N. A case of a solitary metastatic diaphragmatic tumor. Radiat Med. 1998; 16:363–365. PMID: 9862159.4. Griffiths JD, McKinna JA, Rowbotham HD, Tsolakidis P, Salsburg AJ. Carcinoma of the colon and rectum: circulating malignant cells and five-year survival. Cancer. 1973; 31:226–236. PMID: 4683038.
Article5. Philip HG, Santhat N. Principle and practice of surgery for the colon, rectum, and anus. 1999. Missouri: Quality medical publishing, Inc;p. 617–624.6. Kim JC, Kim HC, Jung CS. Carcinoembryonic Antigen-Directed Second Look Operation in Recurrent Colorectal Cancer. Korean J Gastroenterol. 1998; 32:484–491.7. Minton JP, Hoehn JL, Gerber DM. Results of a 400-patient carcinoembryonic antigen second-look colorectal cancer study. Cancer. 1985; 55:1284–1290. PMID: 3971297.
Article8. Hida J, Yasutomi M, Shindoh K. Second-look operation for recurrent colorectal cancer based on carcinoembryonic antigen and imaging techniques. Dis Colon Rectum. 1996; 39:74–79. PMID: 8601361.
Article9. Araki K, Kobayashi M, Ogata T. Colorectal carcinoma metastatic to skeletal muscle. Hepatogastroenterology. 1994; 41:405–408. PMID: 7851845.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Isolated Splenic Metastasis from Colorectal Carcinoma
- TisN0M1 Sigmoid Colon Cancer: A Case Report
- A Case of Cutaneous Metastases to the Face and Scalp from Colon Adenocarcinoma
- Two Cases of Metastatic Adenocarcinoma Developed on Abdominal Skin
- Expression of Osteopontin, ZO-1 and E-cadherin in Adenoma and Adenocarcinoma of the Colon
