Coronary Arteriovenous Fistulas with Aneurysm
- Affiliations
-
- 1Department of Internal Medicine, Gwangju Veterans Hospital, Gwangju, Korea. omoegao@hanmail.net
- KMID: 2116775
- DOI: http://doi.org/10.4068/cmj.2010.46.3.192
Abstract
- Coronary artery fistula with aneurysm is an infrequent vascular anomaly. Echocardiography and angiography have traditionally been used as diagnostic tools for coronary artery fistulas. However, new imaging modalities, such as multi-detector computed tomography (MDCT), can now be used to noninvasively determine the anatomy of an abnormal coronary artery accurately and to facilitate the formulation of appropriate management strategies. In this case, two huge coronary arteriovenous fistulas with aneurysmal changes were observed on 2D-echocardiography and coronary angiography performed on a 72-year-old female. The anatomy of the coronary arteriovenous fistula was then determined in detail by 64-slice MDCT angiography.
Keyword
MeSH Terms
Figure
-
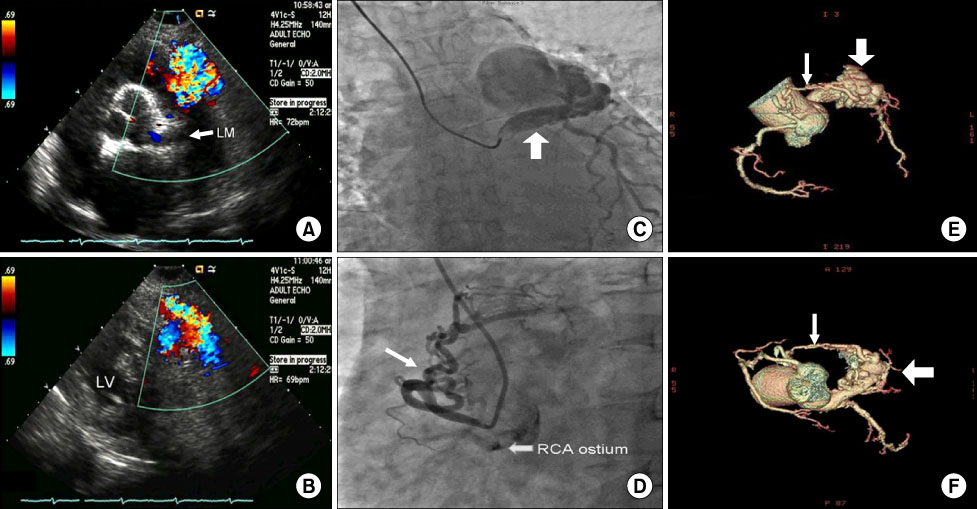
Fig. 1 2D-Echocardiography shows a dilated left main coronary artery and abnormal color flow at the pulmonary valve level (A) and mid-ventricle level (B). Coronary angiography reveals a huge dilated left main artery with aneurysmal formation drained to the pulmonary trunk (wide arrow) (C) and an abnormal fistula originating from the aorta beside the right coronary artery (narrow arrow) (D). A 64-slice multi-detected computed tomography (MDCT) angiograph shows a markedly dilated left main artery and aneurysmal dilatation of an arteriovenous fistula from the left main artery to the pulmonary trunk and an abnormal vessel originating from the right coronary cusp just beside the origin of the right coronary artery drained to the dilated left main artery (E, F).
Reference
-
1. Gowda RM, Vasavada BC, Khan IA. Coronary artery fistulas: clinical and therapeutic considerations. Int J Cardiol. 2006. 107:7–10.
Article2. Versaci F, Del Giudice C, Sperandio M, Simonetti G, Chiariello L. A case of coronary artery fistula visualized by 64-slice multidetector CT. Nat Clin Pract Cardiovasc Med. 2009. 6:57–60.
Article3. Kacmaz F, Isiksalan Ozbulbul N, Alyan O, Maden O, Demir AD, Atak R, et al. Imaging of coronary artery fistulas by multidetector computed tomography: is multidetector computed tomography sensitive? Clin Cardiol. 2008. 31:41–47.
Article4. Shiga Y, Tsuchiya Y, Yahiro E, Kodama S, Kotaki Y, Shimoji E, et al. Left main coronary trunk connecting into right atrium with an aneurysmal coronary artery fistula. Int J Cardiol. 2008. 123:e28–e30.
Article5. Barrera-Ramírez CF, Jiménez-Mazuecos J, Portero Pérez P, Moreno R, Hernández-Antolín R, Alfonso F, et al. Multiple congenital coronary artery fistulae draining into the left ventricle. Arch Cardiol Mex. 2004. 74:45–48.6. Early SA, Meany TB, Fenlon HM, Hurley J. Coronary artery fistula; coronary computed topography--the diagnostic modality of choice. J Cardiothorac Surg. 2008. 3:41.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Dual Coronary Arteriovenous Fistulas Draining into the Coronary Sinus in a Patient with Acute Myocardial Infarction
- Bilateral Congenital Coronary Arteriovenous Fistulas
- A Case of Giant Aneurysm of Coronary Arteriovenous Fistula Treated by Percutaneous Deployment of Embolization Coil
- Giant Aneurysm of a Congenital Coronary Arteriovenous Fistula Arising from the Left Coronary Artery
- A Case of Coronary Arteriovenous Fistula Associated with Pulmonary Artery Aneurysm Confirmed by Multi Detector-Row Helical CT
