Spontaneous Resolution of Post-Traumatic Bilateral Serous Retinal Detachment in Childrens
- Affiliations
-
- 1Department of Ophthalmology, Kang Dong Sacred Heart Hospital, Hallym Medical University, Seoul, Korea. sungpyo@hanafos.com
- KMID: 2110886
- DOI: http://doi.org/10.3341/jkos.2008.49.6.1018
Abstract
-
PURPOSE: We report a case of post.traumatic bilateral serous retinal detachment that resolved spontaneously within a month.
CASE SUMMARY
An 8-year-old male patient presented with post-traumatic bilateral serous retinal detachment and decreased visual acuity. We did not perform any specific treatment. Best corrected visual acuity (BCVA), fluorescein angiography (FA), optical coherence tomography (OCT), and slit lamp examination were used.
CONCLUSIONS
After 1 month, the patient's BCVA improved to 1.0 in both eyes, and serous retinal detachment resolved; FA findings and OCT findings were nearly normal.
MeSH Terms
Figure
-
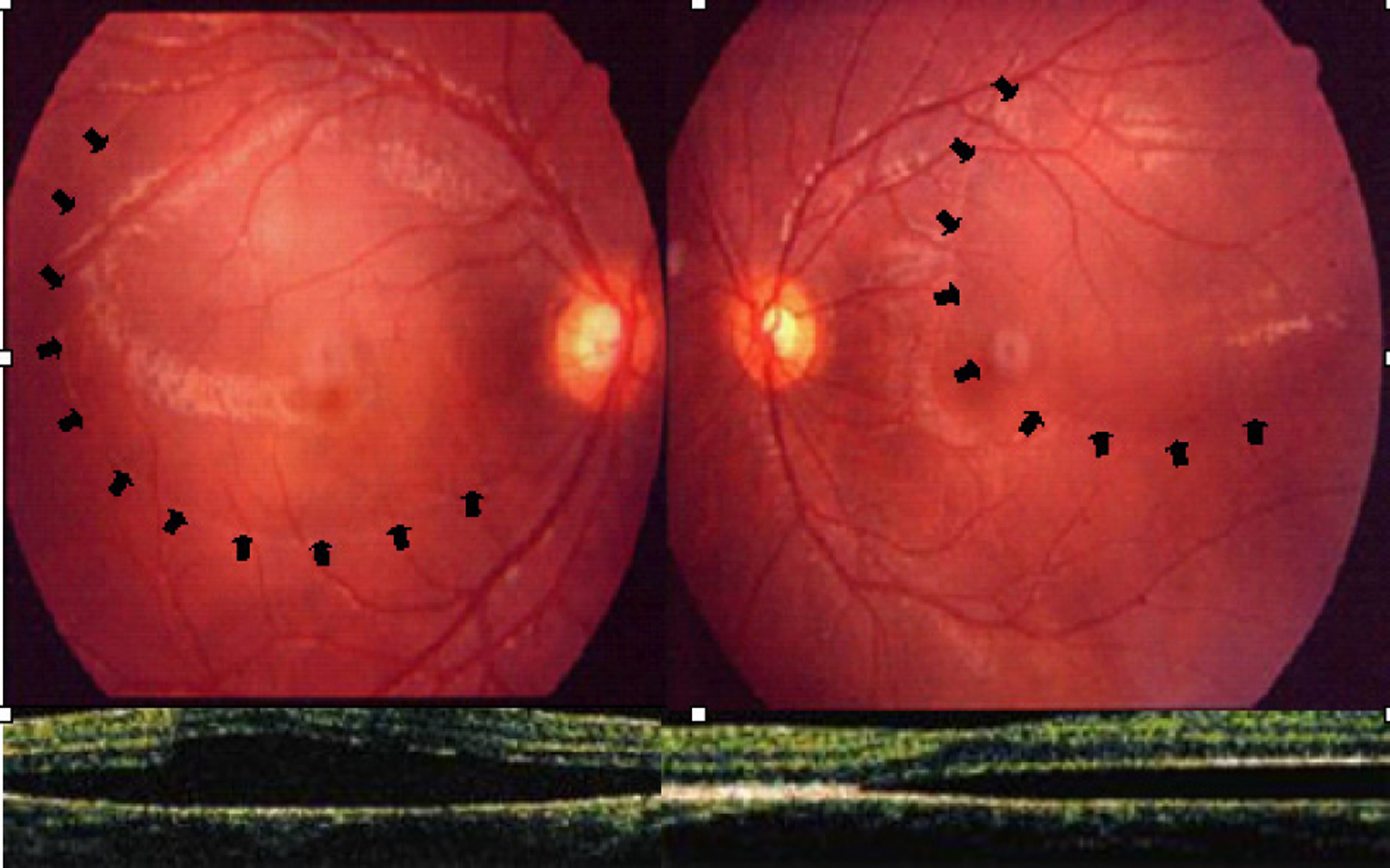
Figure 1. In both eyes, elevated serous lesion at superotemporal area (black arrow lined) was observed. Macular involvement is seen on optical coherence tomography (OCT).
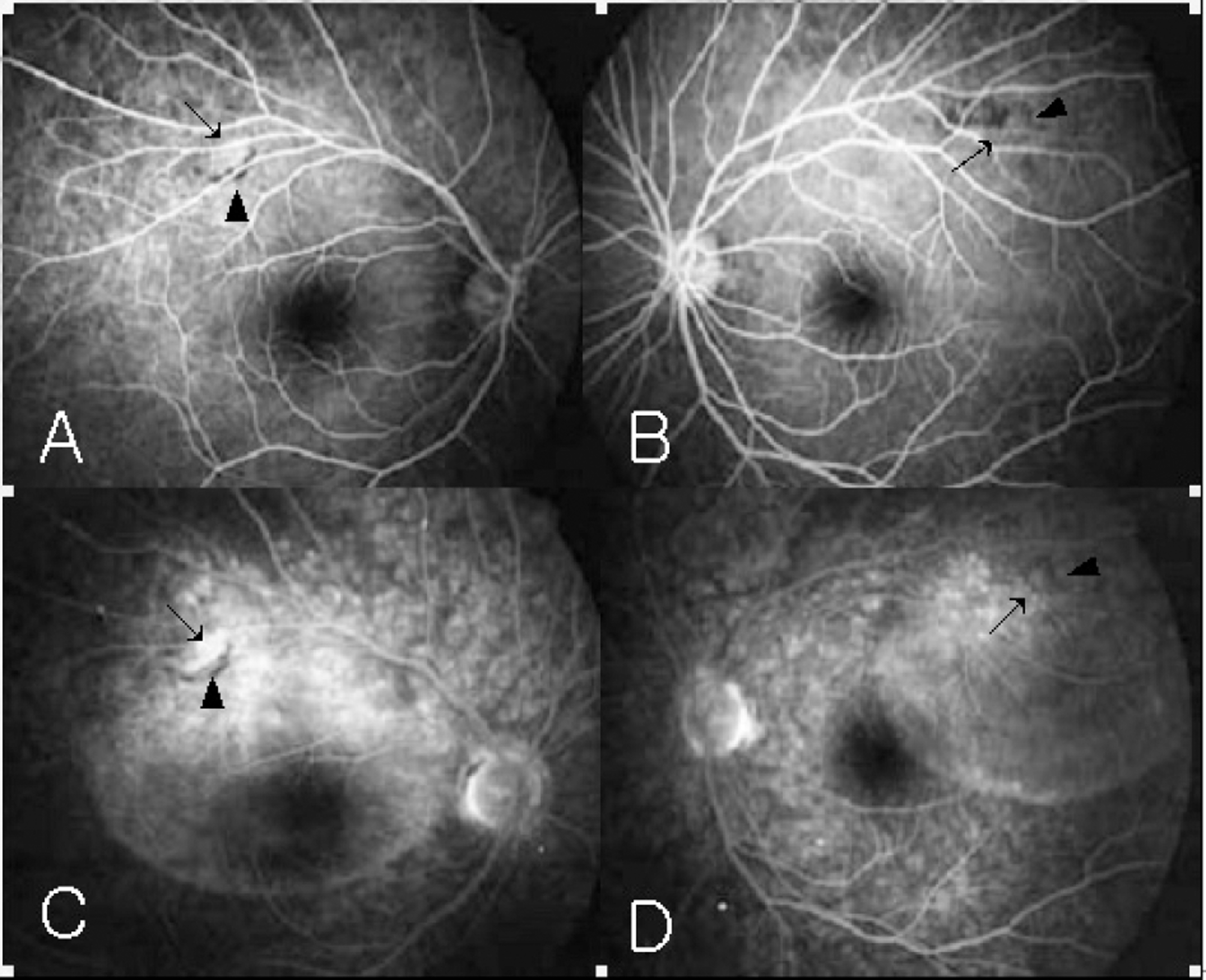
Figure 2. Fluorescein angiographs (FA). (A, B) In the early phase, superotemporal hypofluorescence lesion is seen inside the vascular arcade in both eyes (black arrow head) and hyperfluorescence lesion (black arrow). (C, D) In the late phase, the fluorescence pooling involving macula is seen in both eyes. There are still hypofluorescence lesion (black arrow head). Hyperfluorescence lesion shows slight leakage (black arrow) in the late phase.
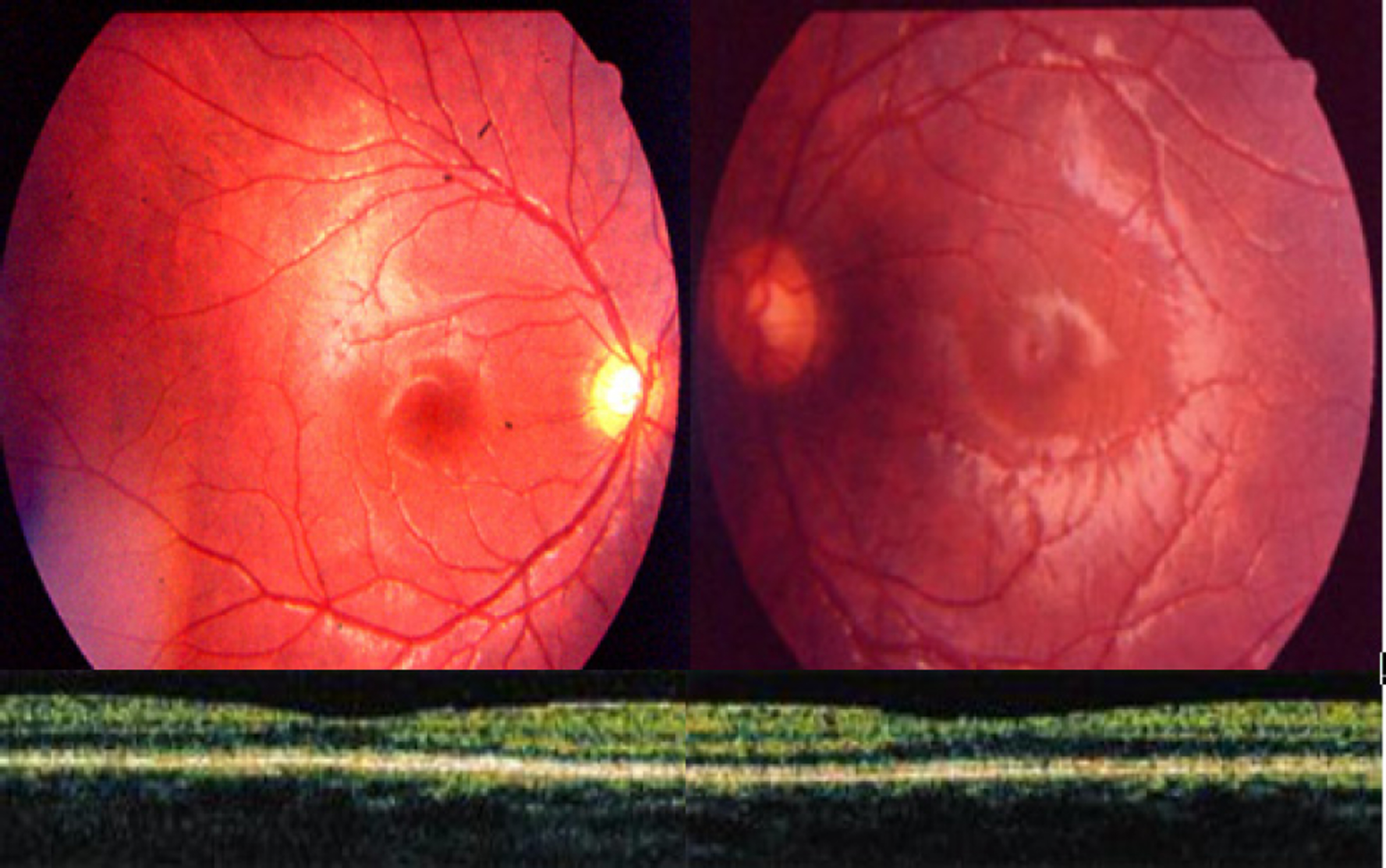
Figure 3. At one month after initial trauma, the elevated serous lesion is no longer seen in both eyes. Also, there is no serous retinal detachment of the macula in both eyes.
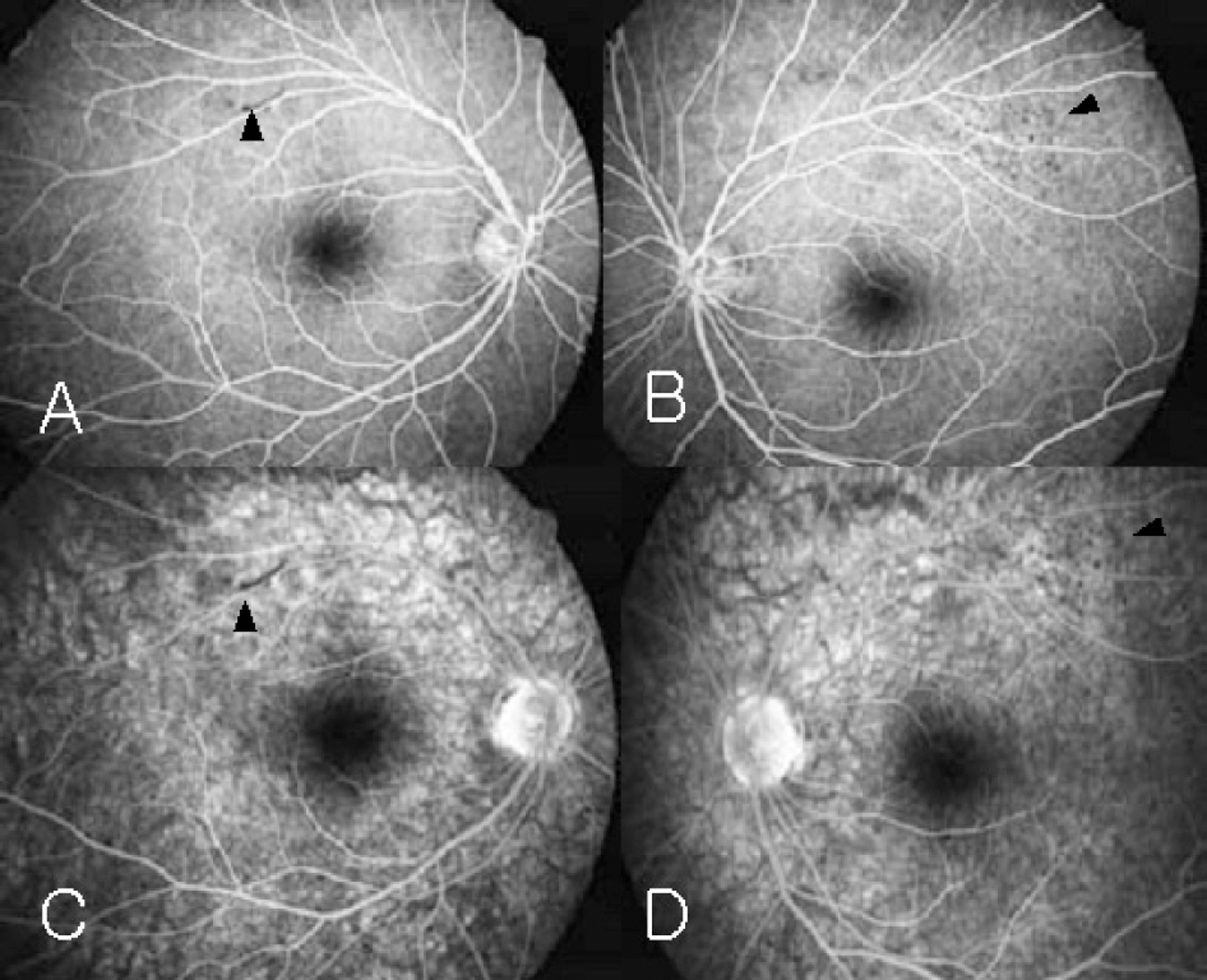
Figure 4. Fluorescein Angiographs (FA) after 1 month. (A, B) Early phase. There still exist hypofluorescence lesions on superotemporal area (black arrow head). (C, D) Late phase. Fluorescein pooling is seen in the late phase. Also, No hyperfluorescence spot is detected.
Cited by 1 articles
-
Two Cases of Serous Retinal Detachment Following Vitrectomy in Patients with Proliferative Diabetic Retinopathy
Jang-Hun Lee, Sa Kang Kim, Sang Beom Han, Seung Jun Lee, Moo Sang Kim
J Korean Ophthalmol Soc. 2017;58(1):98-105. doi: 10.3341/jkos.2017.58.1.98.
Reference
-
References
1. Fisher RF. The influence of age on some ocular basement membranes. Eye. 1987; 1:184–9.
Article2. Casswell AG, Gregor ZJ, Bird AC. The surgical management of uveal effusion syndrome. Eye. 1987; 1:115–9.
Article3. Machemer R. The importance of fluid absorption, traction, intraocular currents, and chorioretinal scars in the therapy of rhegmatogenous retinal detachment. Am J Ophthalmol. 1984; 98:681–93.4. Negi A, Marmor MF. The resorption of subretinal fluid after diffuse damage to the retinal pigment epithelium. Invest Ophthalmol Vis Sci. 1983; 24:1475–9.5. Negi A, Marmor MF. Experimental serous retinal detachment and focal pigment epithelial damage. Arch Ophthalmol. 1984; 102:445–9.
Article6. Van Buskirk EM, Lessell S, Friedman E. Pigmentary epitheliopathy and erythema nodosum. Arch Ophthalmol. 1971; 85:369–72.
Article7. Kohno T, Miki T, Hayashi K. Choroidopathy after blunt trauma to the eye: A fluorescein and Indocyanine angiographic study. Am J Ophthalmol. 1998; 126:248–60.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bilateral Serous Retinal Detachment Associated With Alport's Syndrome
- Effect of Serous Retinal Detachment on the Measurement of Axial Length in Central Serous Chorioretinopathy
- A case of Atypical Central Serous Chorioretinopathy with Bullous Retinal Detachment
- Laser Photocoaculation Treatment in a Case of Circumscribged Choroidal hmangioma Associated with Serous Retinal Detachment
- Takayasu's Arteritis Associated with Serous Retinal Detachment
