A Case of Sarcoidosis Presented as Multiple Conjunctival and Nasal Mucosal Nodule
- Affiliations
-
- 1Department of Ophthalmology, Chonbuk National University, College of Medicine, Chonbuk, Korea. you2ic@paran.com
- 2Department of Ophthalmology, Chonnam National University Medical School, Gwangju, Korea.
- 3Department of Otorhinolaryngology, Chonnam National University Medical School, Gwangju, Korea.
- KMID: 2110883
- DOI: http://doi.org/10.3341/jkos.2008.49.6.1000
Abstract
-
PURPOSE: Sarcoidosis is a noncaseating granulomatous disorder that can affect any organ. In its early phase, sarcoidosis is clinically similar to tuberculosis. We report a case of sarcoidosis diagnosed through ocular and systemic evaluations in a patient who developed multiple conjunctival nodules during antituberculous treatment for nasal mucosal nodules.
CASE SUMMARY
A 37-year-old woman who had been on antituberculosis medications for 9 months because of multiple nasal mucosal nodules was referred for conjunctival hyperemia and the multiple nodules. The ocular examination revealed multiple conjunctival nodules in the upper and lower fornices. Biopsy and systemic evaluations were performed. A conjunctival biopsy specimen showed noncaseating granulomatous inflammation compatible with sarcoidosis. Laboratory tests revealed hypercalciuria and increased levels of ACE. Chest computed tomography showed bilateral hilar and mediastinal lymphadenopathy. Subconjunctival steroid injection was done for the conjunctival nodules and systemic steroid treatment was started as well. Complete resolution of conjunctival lesions was obtained.
CONCLUSIONS
In cases of chronic, multiple conjunctival and nasal mucosal nodules, sarcoidosis should be considered in the differential diagnosis.
Keyword
MeSH Terms
Figure
-
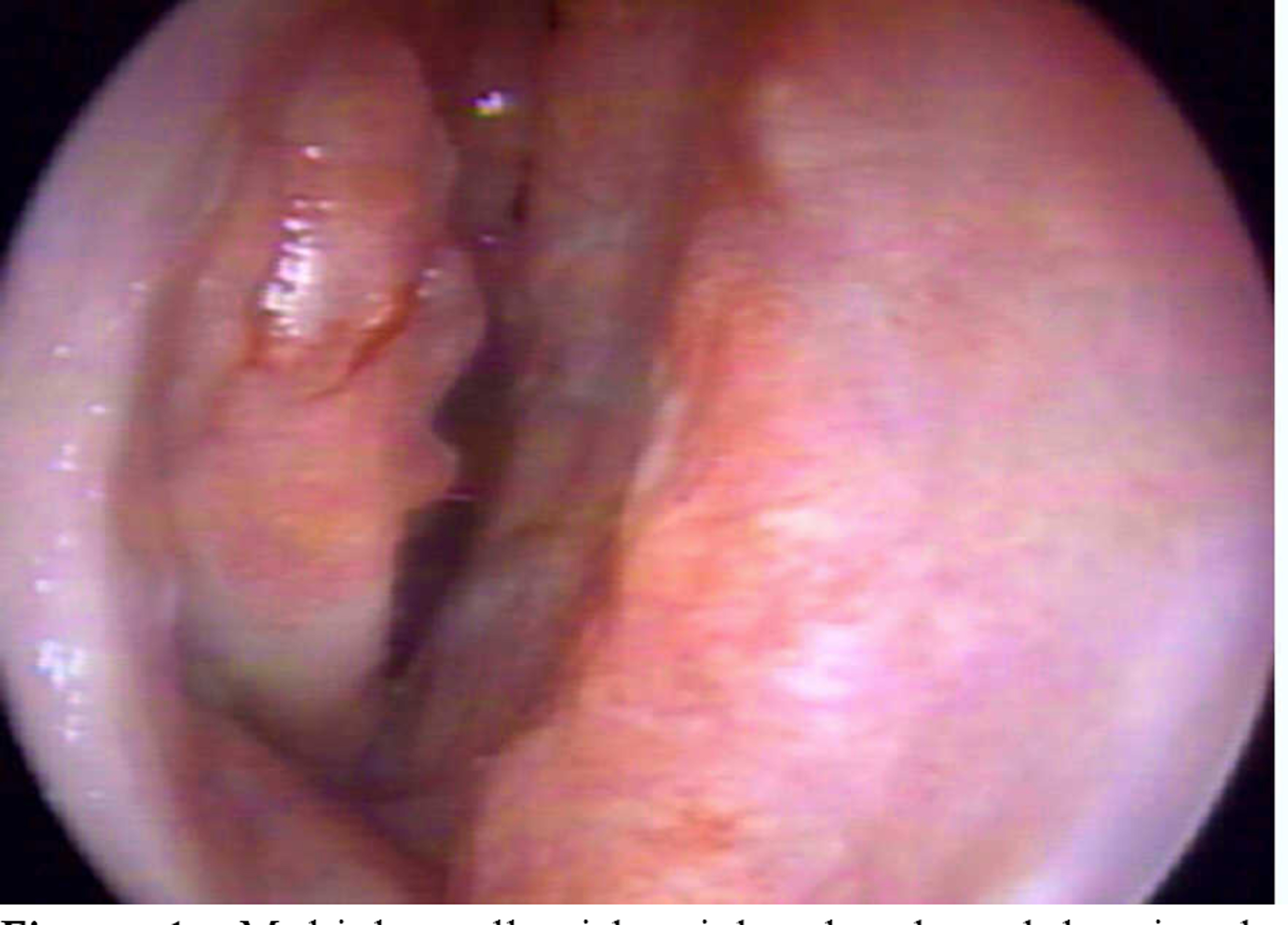
Figure 1. Multiple yellowish pink-colored nodules in the nasal septum and inferior turbinate.

Figure 2. Pretreatment and posttreatment anterior segment photographs of the left eye. (A&B) Multiple yellowish nodules on the lateral canthus, movable and elevated smooth nodules in the upper fornix at the initial visit. (C&D) Six months after treatment, the bulbar conjunctiva and fornix were cleared.
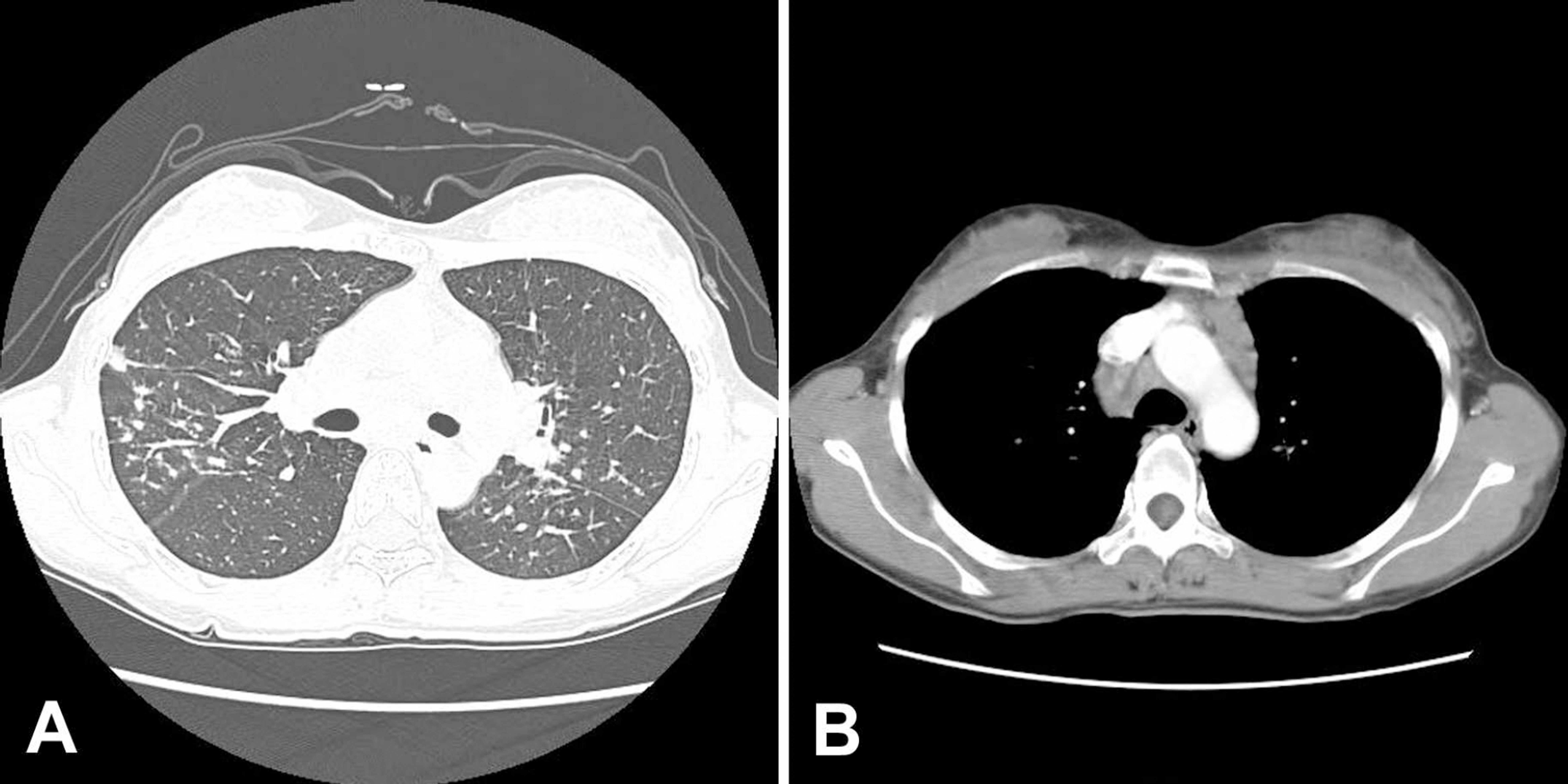
Figure 3. Chest CT findings. (A) Multiple small nodules with some peribronchovascular distribution, confluent densities, and small branching structure in both lung. (B) Multiple small and enlarged conglomerate lymphadenopathies in left supraclavicular area, both sides of the mediastinum, subcarinal, both hilar, and both interlobar nodal areas.
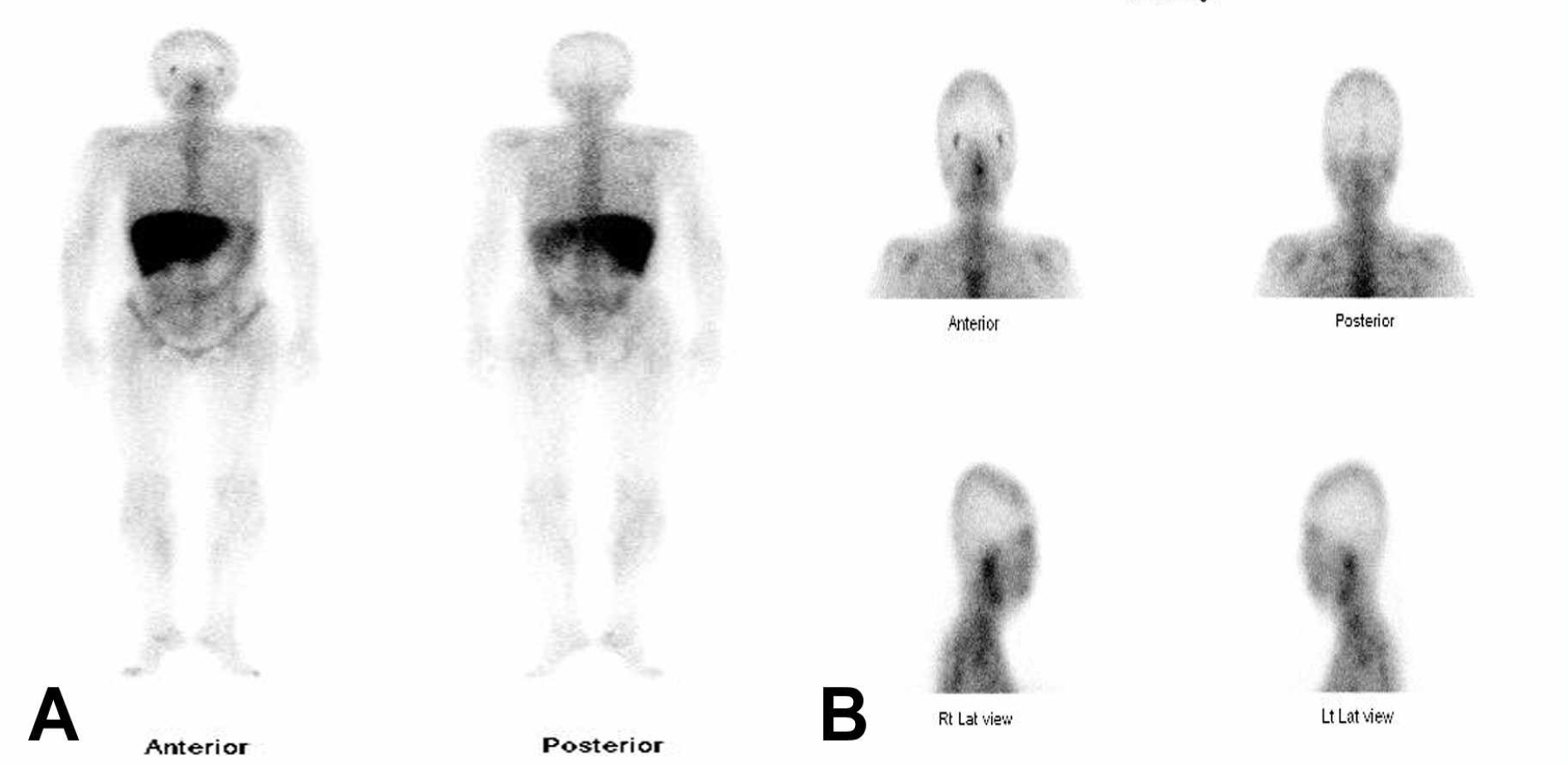
Figure 4. 67-Ga Scan images demonstrate normal galium-67 citrate accumulation in the liver (A), both lacrimal glands, nasal cavity and bone marrow (B).

Figure 5. Histologic findings show noncaseating epitheloid granuloma and composition of epithelioid histiocytes, Langerhans' cell and lymphocytes (H&E stain, ×200).

Figure 6. Posttreatment chest CT demonstrate more decreased, but still remained multiple small lymphoadenopathy.
Cited by 1 articles
-
A Case of Isolated Orbital Sarcoidosis
Jin Sung Park, Mi Sun Kwak
J Korean Ophthalmol Soc. 2014;55(10):1549-1553. doi: 10.3341/jkos.2014.55.10.1549.
Reference
-
References
1. Dios E, Saornil MA, Herreras JM. Conjunctival biopsy in the diagnosis of ocular sarcoidosis. Ocul Immunol Inflamm. 2001; 9:59–64.
Article2. Evans M, Sharma O, Labree L. . A differences in clinical findings between caucasians and african americans with biopsy-proven sarcoidosis. Ophthalmology. 2007; 114:325–33.3. Jabs DA, Johns CJ. Ocular involvement in chronic sarcoidosis. Am J Ophthalmol. 1986; 102:297–301.
Article4. Smith JA, Foster CS. Sarcoidosis and its ocular manifestations. Int Ophthalmol Clin. 1996; 36:109–25.
Article5. Dresner MS, Brecher R, Henkind P. Ophthalmology consultation in the diagnosis and treatment of sarcoidosis. Arch Intern Med. 1986; 146:301–4.
Article6. Obenauf CD, Shaw HE, Sydnor CF, Klintworth GK. Sarcoidosis and its ophthalmic manifestation. Am J Ophthalmol. 1978; 86:648–55.7. Bonfioli AA, Orefice F. Sarcoidosis. Semin Ophthalmol. 2005; 20:177–82.
Article8. Kim YJ, Kim YD. A case of scar sarcoidosis of the eyelid. Korean J Ophthalmol. 2006; 20:238–40.
Article9. Ko DA, Kim BJ. Sarcoidosis, presented as recurrent eyelid masses. J Korean Ophthalmol Soc. 2004; 45:1590–5.10. Lee DY, Kim DH, Yu SY, Kwak HW. A case of sarcoidosis misdiagnosed as tuberculosis in the early phase. J Korean Ophthalmol Soc. 2004; 45:438–43.11. Lee TH, Kim YJ, Sin DH. Case report: ocular sarcoidosis. J Korean Ophthalmol Soc. 1993; 34:687–91.12. Cho NC, Ahn HS. A case of palpebral sarcoidosis associated with granulomatous uveitis. J Korean Ophthalmol Soc. 1990; 31:819–23.13. Kim KS, Choi BC, Kim HJ. . A case of sarcoidosis associated with uveitis and vitreous hemorrhage. J Korean Ophthalmol Soc. 1988; 29:433–9.14. Sohn MS, Kim JD, Cha OJ. . A case of sarcoidosis associated with granulomatous uveitis. J Korean Ophthalmol Soc. 1967; 8:11–6.15. De Shazo RD, O’Brien MM, Justice WK, Pitcock J. Diagnostic criteria for sarcoidosis of the sinuses. J Allergy Clin Immunol. 1999; 103:789–95.16. Baughman RP, Lower EE. du Bois RM. Sarcoidosis. Lancet. 2003; 361:1111–8.17. Shah UK, White JA, Gooey JE, Hybels RL. Otolaryngologic manifestations of sarcoidosis: presentation and diagnosis. Laryngoscope. 1997; 107:67–75.
Article18. Damrose EJ, Huang RY, Abemayor E. Endoscopic diagnosis of sarcoidosis in a patient presenting with bilateral exophthalmos and pansinusitis. Am J Rhinol. 2000; 14:241–4.
Article19. Lee JH, Kim NS, Cho JH, Lee YS. A case of ethmoidal sarcoidosis Korean. J Otorhinolaryngol‐ Head Neck Surg. 2007; 50:716–8.20. Fernaridez Fabrellas E. Epidemiology of sarcoidosis. Arch Bronconeumol. 2007; 43:92–100.21. Zeitlin JF, Tami TA, Baughman R, Winget D. Nasal and sinus manifestations of sarcoidosis. Am J Rhinol. 2000; 14:157–61.
Article22. James DG, Barter S, Jash D, MacKinnon DM, Carstairs LS. Sarcoidosis of upper respiratory tract (SURT). J Laryngol Otol. 1982; 96:711–8.23. Wilson R, Lund V, Sweatman M. . Upper respiratory tract involvement in sarcoidosis and its management. Eur Respir J. 1988; 1:269–72.24. Aubart FC, Ouayoun M, Brauner M. . Sinonasal involvement in sarcoidosis. A case‐ control study of 20 patients. Medicine. 2006; 85:365–71.
Article25. Braun JJ, Gentine A, Pauli G. Sinonasal sarcoidosis: review and report of fifteen cases. Laryngoscope. 2004; 114:1960–3.
Article26. Dithmar S, Waring GO III, Goldblum TA, Grossniklaus HE. Conjunctival deposits as an initial manifestation of sarcoidosis. Am J Ophthalmol. 1999; 128:361–2.
Article27. Akpek EK, Ilhan-Sarac O, Green WR. Topical cyclosporin in the treatment of chronic sarcoidosis. Arch Ophthalmol. 2003; 121:1333–5.28. Schilgen G, Sundmacher R, Pomjanski N. . Bilateral large conjunctival tumors as primary manifestation of sarcoidosis- successful treatment with steroid‐ depot‐ injection. Klin Monatsbl Augenheikd. 2006; 223:326–9.29. Jones onesN. Sarcoidosis and uveitis. Ophthalmol Clin North Am. 2002; 15:319–26.
Article
