Measurement Discrepancy of Sagittal Parameters between Plain Radiography and 3D Computed Tomography in Thoracolumbar and Lumbar Fractures
- Affiliations
-
- 1Department of Orthopedic Surgery, Chungbuk National University College of Medicine, Cheongju, Korea. ymkim@chungbuk.ac.kr
- KMID: 2106648
- DOI: http://doi.org/10.4055/jkoa.2012.47.3.198
Abstract
- PURPOSE
For decision making in the management of vertebral fractures such as operation or not, sagittal parameters like Cobb angle and wedge compression ratio are important. Plain radiography had been the only image tool for measuring such parameters until 3D computed tomography (CT) became popular recently. In this study, we investigated the measurement discrepancy between plain radiography and 3D CT.
MATERIALS AND METHODS
Plain radiography and 3D CT of 45 thoracolumbar and lumbar fracture patients (male=21, female=24) were evaluated. We measured sagittal angle and vertebral height on lateral radiography and sagittal CT. Sagittal angle was measured between the upper body and lower body of fractured vertebrae. Anterior and posterior heights were measured to assess anteriorposterior (AP) wedge ratio.
RESULTS
The sagittal angle of plain radiography (13.1+/-14.3degrees) was significantly larger than that of 3D CT (8.2+/-13.0degrees) by 4.9degrees (p<0.001). AP wedge ratio of plain radiography was on average 65+/-17%, which was significantly lower than the 3D CT (73+/-17%) by 8% (p<0.001). The severer the initial kyphotic deformity, the more discrepancy of results between the two methods was observed.
CONCLUSION
Significant discrepancy was observed in sagittal features of fractured vertebra between plain radiography and 3D CT. Measured values of plain radiography showed more kyphotic features of the fractured body.
Figure
-
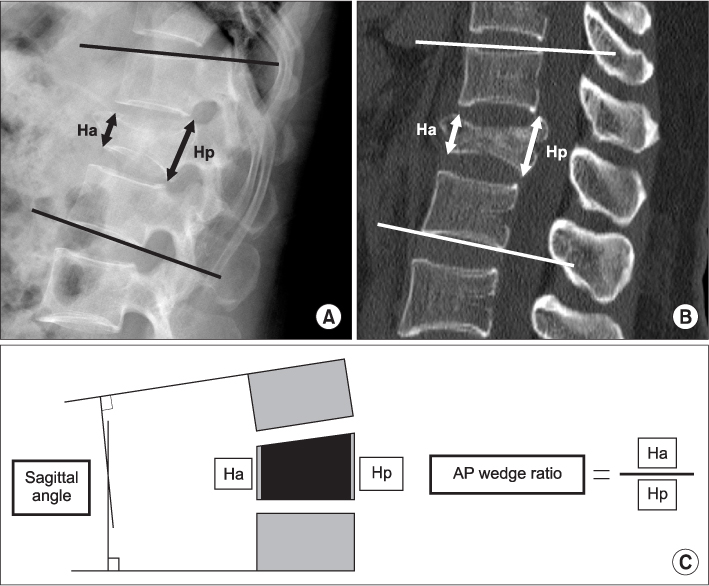
Figure 1 Measurement method of sagittal angle and AP wedge ratio in plain radiograph (A), mid-sagittal plane of 3D CT (B) and schematic illustration (C). Sagittal angle is Cobb angle between upper end plate of upper body and lower end plate of lower body. AP wedge ratio is anterior body height divided by posterior body height (Ha/Hp) of fractured vertebra. AP, anterior-posterior; CT, computed tomography; Ha, anterior height; Hp, posterior height.
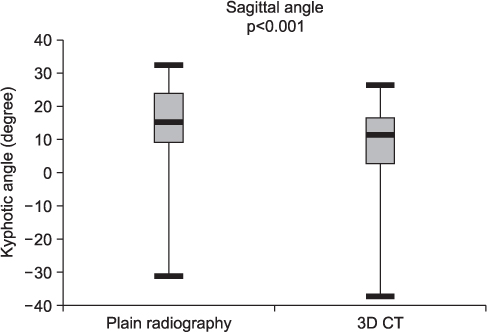
Figure 2 Comparison between plain radiography and 3D CT in sagittal angle. The sagittal angle of plain radiography (13.1±14.3°) was significantly larger than that of 3D CT (8.2±13.0°) by 4.9° (p<0.001). CT, computed tomography.

Figure 3 Plain radiograph (A) and sagittal CT (B) of a 28-year-old female patient. In plain radiograph, sagittal angle is 29.3° and AP wedge ratio is 57%. Sagittal angle and AP wedge ratio of 3D CT are 21.2° and 67% respectively. Sagittal parameters of plain radiograph are more kyphotic than 3D CT. CT, computed tomography; AP, anterior-posterior.
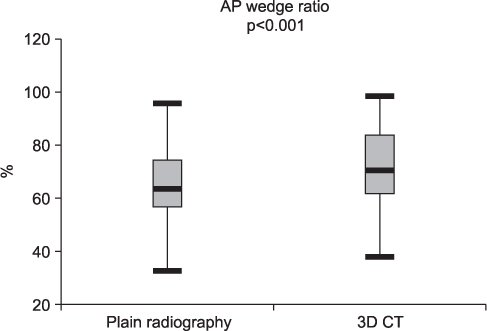
Figure 4 Discrepancy between plain radiograph and 3D CT in AP wedge ratio. AP wedge ratio of plain radiograph is lower than 3D CT (p<0.001). CT, computed tomography; AP, anterior-posterior.
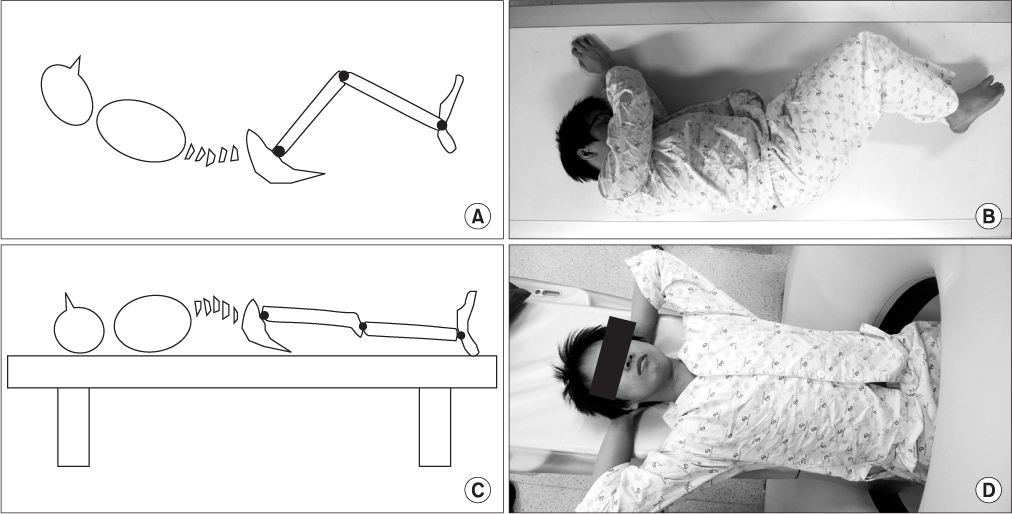
Figure 5 Schematic illustrations and photographs of position when obtaining plain lateral radiography (A, B) and 3D computed tomography (C, D).
Reference
-
1. Tadmor R, Davis KR, Roberson GH, New PF, Taveras JM. Computed tomographic evaluation of traumatic spinal injuries. Radiology. 1978. 127:825–827.
Article2. McAfee PC, Yuan HA, Fredrickson BE, Lubicky JP. The value of computed tomography in thoracolumbar fractures. An analysis of one hundred consecutive cases and a new classification. J Bone Joint Surg Am. 1983. 65:461–473.
Article3. Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979. 86:420–428.
Article4. Cobb JR. The problem of the primary curve. J Bone Joint Surg Am. 1960. 42:1413–1425.
Article5. Lucey BC, Stuhlfaut JW, Hochberg AR, Varghese JC, Soto JA. Evaluation of blunt abdominal trauma using PACS-based 2D and 3D MDCT reformations of the lumbar spine and pelvis. AJR Am J Roentgenol. 2005. 185:1435–1440.
Article6. Ballock RT, Mackersie R, Abitbol JJ, Cervilla V, Resnick D, Garfin SR. Can burst fractures be predicted from plain radiographs? J Bone Joint Surg Br. 1992. 74:147–150.
Article7. Kim YM, Kim DS, Choi ES, et al. Bone & soft tissue injuries diagnosed by magnetic resonance imaging in thoracolumbar fractures. J Korean Fract Soc. 2004. 17:184–190.8. Berry GE, Adams S, Harris MB, et al. Are plain radiographs of the spine necessary during evaluation after blunt trauma? Accuracy of screening torso computed tomography in thoracic/lumbar spine fracture diagnosis. J Trauma. 2005. 59:1410–1413.
Article9. Diaz JJ Jr, Cullinane DC, Altman DT, et al. EAST Practice Management Guideline Committee. Practice management guidelines for the screening of thoracolumbar spine fracture. J Trauma. 2007. 63:709–718.
Article10. Epstein O, Ludwig S, Gelb D, Poelstra K, O'Brien J. Comparison of computed tomography and plain radiography in assessing traumatic spinal deformity. J Spinal Disord Tech. 2009. 22:197–201.
Article11. Street J, Lenehan B, Albietz J, Bishop P, Dvorak M, Fisher C. Spine Trauma Study Group. Intraobserver and interobserver reliabilty of measures of kyphosis in thoracolumbar fractures. Spine J. 2009. 9:464–469.
Article12. Di Chiro G, Schellinger D. Computed tomography of spinal cord after lumbar intrathecal introduction of metrizamide (computer-assisted myelography). Radiology. 1976. 120:101–104.
Article13. Brant-Zawadzki M, Miller EM, Federle MP. CT in the evaluation of spine trauma. AJR Am J Roentgenol. 1981. 136:369–375.
Article14. Roub LW, Drayer BP. Spinal computed tomography: limitations and applications. AJR Am J Roentgenol. 1979. 133:267–273.
Article15. Willén J, Lindahl S, Irstam L, Nordwall A. Unstable thoracolumbar fractures A study by CT and conventional roentgenology of the reduction effect of Harrington instrumentation. Spine (Phila Pa 1976). 1984. 9:214–219.16. Chance GQ. Note on a type of flexion fracture of the spine. Br J Radiol. 1948. 21:452.
Article17. Handelberg F, Bellemans MA, Opdecam P, Casteleyn PP. The use of computerised tomographs in the diagnosis of thoracolumbar injury. J Bone Joint Surg Br. 1981. 63:337–341.
Article18. Post MJ, Green BA, Quencer RM, Stokes NA, Callahan RA, Eismont FJ. The value of computed tomography in spinal trauma. Spine (Phila Pa 1976). 1982. 7:417–431.
Article19. Hauser CJ, Visvikis G, Hinrichs C, et al. Prospective validation of computed tomographic screening of the thoracolumbar spine in trauma. J Trauma. 2003. 55:228–234.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of the Size of the Posterior Malleolar Fragment in Trimalleolar Ankle Fractures Measured Using Lateral Plain Radiography and Three-Dimensional Computed Tomography
- A Clinical Study of Unstable Fractures and Fracture-Dislocations of the Thoracolumbar Spine - Comparision Between Holdsworth, Denis and McAfee Classification -
- Three-Dimensional Computed Tomography of Acetabular Fractures
- Three-dimensional reformation of computed tomography in the nasal bone fractures
- Measurement of Vertebral Compression and Kyphosis in the Thoracolumbar and Lumbar Fractures
