Efficacy of Octreotide LAR in Acromegalic Patients
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2100465
- DOI: http://doi.org/10.3803/jkes.2005.20.4.344
Abstract
-
BACKGROUND: Octreotide(OC)-LAR is a long-acting preparation of octreotide which has been effectively used to suppress GH/IGF-1 hypersecretion in acromegalic patients. The clinical response, biochemical outcomes, and safety of OC-LAR were evaluated in 27 active acromegalic patients.
METHOD: 27patients with an active disease status (according to the clinical picture, GH >5microgram/L and elevated age-matched IGF-1), and previously treated with bromocriptine after surgery, comprised the study population. OC-LAR was given(20mg, i.m., every 4 week for 3 injections, then the doses were titrated individually) and the acromegalic symptoms and adverse reactions recorded. The serum levels of GH and IGF-1 were evaluated every 12 week. The acromegalic symptoms including headache, fatigue and arthralgia, improved in all patients.
RESULTS
Gastrointestinal side effects were transient and mild. The levels of GH significantly decreased, from 8.9+/-3.5 to 2.9+/-2.2 microgram/L at 12 weeks(P<0.001, vs. baseline), to 2.9+/-2.1microgram/L after 24 weeks(P<0.001) and to 2.5 +/-1.3microgram/L at 48 weeks(P<0.001). The levels of IGF-1 significantly decreased, from 753.7+/-213.6 to 429.7+/-253.4 microgram/L at 12 weeks(P<0.001, vs. at baseline), to 405.7+/-213.3microgram/L at 24 weeks(P <0.001) and to 348.9+/-144.7microgram/L at 48 weeks(P<0.001). The safelevel of GH is less than 2.5microgram/L and normal age-matched IGF-1 levels were achieved in 63 and 52% of the patients, respectively.
CONCLUSION
Octreotide-LAR was well tolerated and effective as an adjuvant treatment in lowering the levels of GH and IGF-1 in active acromegalic patients.
MeSH Terms
Figure
-
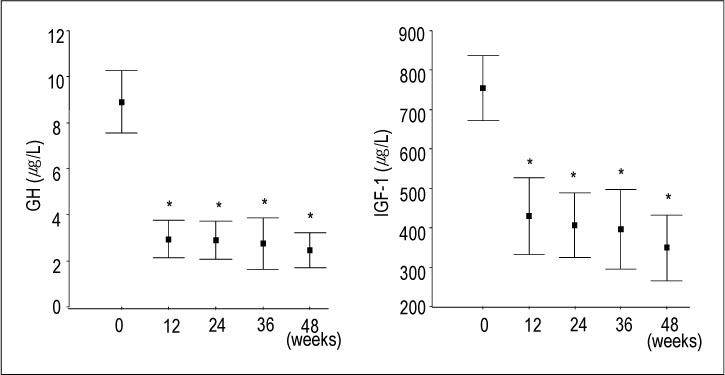
Fig. 1 GH (a) and IGF-1 (b) levels (mean ± SD) during treatment. GH and IGF-1 levels decreased significantly at 12 weeks and progressively suppressed. *P< 0.01 vs. basal level
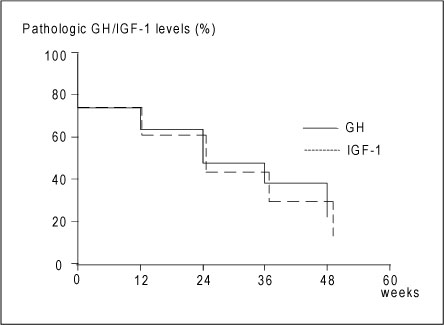
Fig. 2 Kaplan-Meier analysis for achievement of safe GH levels and IGF-1 normalization. The rate of safe GH (<2.5 µg/L) and IGF-1 normalization were 78% and 88% at 48 weeks

Fig. 3 Individual GH level (a) and IGF-1 levels (b) at basal (upper line) and final (lower line) on OC-LAR
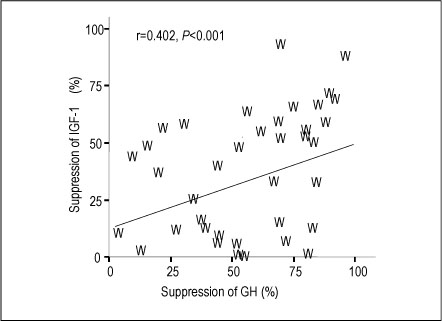
Fig. 4 Correlation between the responses of GH and IGF-1 on OC-LAR. There is positive correlation between the suppression (%) of GH and IFG-1 during treatment (r=0.402, P<0.001)
Cited by 2 articles
-
Comparison of the Efficacy of Octreotide Long-acting Repeatable and Lanreotide Autogel in Acromegalic Patients (
J Korean Endocr Soc 25:37–45, 2010)
Seul Young Kim, Dohee Kim
Endocrinol Metab. 2010;25(2):159-160. doi: 10.3803/EnM.2010.25.2.159.Comparison of the Efficacy of Octreotide Long-acting Repeatable and Lanreotide Autogel in Acromegalic Patients
Seul young Kim, Dohee Kim
J Korean Endocr Soc. 2010;25(1):37-45. doi: 10.3803/jkes.2010.25.1.37.
Reference
-
1. Wright AD, Hill DM, Lowy C, Fraser TR. Mortality in acromegaly. Q J Med. 1970. 39:1–16.2. Growth Hormone Research Society. Pituitary Society. Biochemical assessment and long-term monitoring in patients with acromegaly: statement from a joint consensus conference of the Growth Hormone Research Society and the Pituitary Society. J Clin Endocrinol Metab. 2004. 89:3099–3102.3. Melmed S. Octreotide stimulates insulin-like growth factor binding protein-1: a novel mechanism of drug action on acromegaly. Semin Oncol. 1994. 21:65–69.4. Rajasoorya C, Holdaway IM, Wrightson P, Scott DJ, Ibbertson HK. Determinants of clinical outcome and survival in acromegaly. Clin Endocrinol (Oxf). 1994. 41:95–102.5. Melmed S. Acromegaly. N Engl J Med. 1990. 322:966–977.6. Melmed S, Jackson I, Kleinberg D, Klibanski A. Current treatment guidelines for acromegaly. J Clin Endocrinol Metab. 1998. 83:2646–2652.7. Giustina A, Barkan A, Casanueva FF, Cavagnini F, Frohman L, Ho K, Veldhuis J, Wass J, Von Werder K, Melmed S. Criteria for cure of acromegaly: a consensus statement. J Clin Endocrinol Metab. 2000. 85:526–529.8. Freda PU, Wardlaw SL, Post KD. Long-term endocrinological follow-up evaluation in 115 patients who underwent transsphenoidal surgery for acromegaly. J Neurosurg. 1998. 89:353–358.9. Stewart PM, Kane KF, Stewart SE, Lancranjan I, Sheppard MC. Depot long-acting somatostatin analog (Sandostatin-LAR) is an effective treatment for acromegaly. J Clin Endocrinol Metab. 1995. 80:3267–3272.10. Van der Lely AJ, de Herder WW, Lamberts SW. The role of radiotherapy in acromegaly. J Clin Endocrinol Metab. 1997. 82:3185–3186.11. Jaffe CA, Barkan AL. Treatment of acromegaly with dopamine agonists. Endocrinol Metab Clin North Am. 1992. 21:713–735.12. Abs R, Verhelst J, Maiter D, Van Acker K, Nobels F, Coolens JL, Mahler C, Beckers A. Cabergoline in the treatment of acromegaly: a study in 64 patients. J Clin Endocrinol Metab. 1998. 83:374–378.13. Amato G, Mazziotti G, Rotondi M, Iorio S, Doga M, Sorvillo F, Manganella G, Di Salle F, Giustina A, Carella C. Long-term effects of lanreotide SR and octreotide LAR on tumour shrinkage and GH hypersecretion in patients with previously untreated acromegaly. Clin Endocrinol (Oxf). 2002. 56:65–71.14. Bevan JS, Atkin SL, Atkinson AB, Bouloux PM, Hanna F, Harris PE, James RA, McConnell M, Roberts GA, Scanlon MF, Stewart PM, Teasdale E, Turner HE, Wass JA, Wardlaw JM. Primary medical therapy for acromegaly: an open, prospective, multicenter study of the effects of subcutaneous and intramuscular slow-release octreotide on growth hormone, insulin-like growth factor-I, and tumor size. J Clin Endocrinol Metab. 2002. 87:4554–4563.15. Colao A, Ferone D, Marzullo P, Cappabianca P, Cirillo S, Boerlin V, Lancranjan I, Lombardi G. Long-term effects of depot long-acting somatostatin analog octreotide on hormone levels and tumor mass in acromegaly. J Clin Endocrinol Metab. 2001. 86:2779–2786.16. Swearingen B, Barker FG 2nd, Katznelson L, Biller BM, Grinspoon S, Klibanski A, Moayeri N, Black PM, Zervas NT. Long-term mortality after transsphenoidal surgery and adjunctive therapy for acromegaly. J Clin Endocrinol Metab. 1998. 83:3419–3426.17. Gittoes NJ, Sheppard MC, Johnson AP, Stewart PM. Outcome of surgery for acromegaly--the experience of a dedicated pituitary surgeon. Qjm. 1999. 92:741–745.18. Peacey SR, Shalet SM. Growth hormone pulsatility in acromegaly following radiotherapy. Pituitary. 1999. 2:63–69.19. Attanasio R, Epaminonda P, Motti E, Giugni E, Ventrella L, Cozzi R, Farabola M, Loli P, Beck-Peccoz P, Arosio M. Gamma-knife radiosurgery in acromegaly: a 4-year follow-up study. J Clin Endocrinol Metab. 2003. 88:3105–3112.20. Al-Maskari M, Gebbie J, Kendall-Taylor P. The effect of a new slow-release, long-acting somatostatin analogue, lanreotide, in acromegaly . Clin Endocrinol (Oxf). 1996. 45:415–421.21. Turner HE, Vadivale A, Keenan J, Wass JA. A comparison of lanreotide and octreotide LAR for treatment of acromegaly. Clin Endocrinol (Oxf). 1999. 51:275–280.22. Gillis JC, Noble S, Goa KL. Octreotide long-acting release (LAR). A review of its pharmacological properties and therapeutic use in the management of acromegaly. Dru. s. 1997. 53:681–699.23. Lamberts SW, van der Lely AJ, de Herder WW, Hofland LJ. Octreotide. N Engl J Med. 1996. 334:246–254.24. Cozzi R, Attanasio R, Montini M, Pagani G, Lasio G, Lodrini S, Barausse M, Albizzi M, Dallabonzana D, Pedroncelli AM. Four-year treatment with octreotide-long-acting repeatable in 110 acromegalic patients: predictive value of short-term results? J Clin Endocrinol Metab. 2003. 88:3090–3098.25. Lamberts SW. The role of somatostatin in the regulation of anterior pituitary hormone secretion and the use of its analogs in the treatment of human pituitary tumors. Endocr Rev. 1988. 9:417–436.26. Lamberts SW, Zweens M, Klijn JG, van Vroonhoven CC, Stefanko SZ, Del Pozo E. The sensitivity of growth hormone and prolactin secretion to the somatostatin analogue SMS 201-995 in patients with prolactinomas and acromegaly. Clin Endocrinol (Oxf). 1986. 25:201–212.27. Van der Lely AJ, Harris AG, Lamberts SW. The sensitivity of growth hormone secretion to medical treatment in acromegalic patients: influence of age and sex. Clin Endocrinol (Oxf). 1992. 37:181–185.28. Acromegaly Therapy Consensus Development Panel. Consensus statement: Benefits versus risks of medical therapy for acromegaly. Am J Med. 1994. 97:468–473.29. Montini M, Gianola D, Pagani MD, Pedroncelli A, Caldara R, Gherardi F, Bonelli M, Lancranjan I, Pagani G. Cholelithiasis and acromegaly: therapeutic strategies. Clin Endocrinol (Oxf). 1994. 40:401–406.30. Dowling RH, Hussaini SH, Murphy GM, Besser GM, Wass JA. Gallstones during octreotide therapy. Metabolism. 1992. 41:22–33.31. Caron P, Morange-Ramos I, Cogne M, Jaquet P. Three year follow-up of acromegalic patients treated with intramuscular slow-release lanreotide. J Clin Endocrinol Metab. 1997. 82:18–22.33. Van der Lely AJ, Hutson RK, Trainer PJ, Besser GM, Barkan AL, Katznelson L, Klibanski A, Herman-Bonert V, Melmed S, Vance ML, Freda PU, Stewart PM, Friend KE, Clemmons DR, Johannsson G, Stavrou S, Cook DM, Phillips LS, Strasburger CJ, Hackett S, Zib KA, Davis RJ, Scarlett JA, Thorner MO. Long-term treatment of acromegaly with pegvisomant, a growth hormone receptor antagonist. Lancet. 2001. 358:1754–1759.34. Wagenaar AH, Harris AG, Van der Lely AJ, Lamberts SW. Dynamics of the acute effects of octreotide, bromocriptine and both drugs in combination on growth hormone secretion in acromegaly. Acta Endocrinol (Copenh). 1991. 125:637–642.35. Freda PU, Post KD, Powell JS, Wardlaw SL. Evaluation of disease status with sensitive measures of growth hormone secretion in 60 postoperative patients with acromegaly. J Clin Endocrinol Metab. 1998. 83:3808–3816.36. Dimaraki EV, Jaffe CA, DeMott-Friberg R, Chandler WF, Barkan AL. Acromegaly with apparently normal GH secretion: implications for diagnosis and follow-up. J Clin Endocrinol Metab. 2002. 87:3537–3542.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of the Efficacy of Octreotide Long-acting Repeatable and Lanreotide Autogel in Acromegalic Patients
- Sustained Maintenance of Normal Insulin-like Growth Factor-I during Pregnancy and Successful Delivery in an Acromegalic Patient with Octreotide-LAR(R) Treatment
- Comparison of the Efficacy of Octreotide Long-acting Repeatable and Lanreotide Autogel in Acromegalic Patients
- Letter: Comparison of the Efficacy of Octreotide Long-acting Repeatable and Lanreotide Autogel in Acromegalic Patients (J Korean Endocr Soc 25:37-45, 2010)
- Response: Comparison of the Efficacy of Octreotide Long-acting Repeatable and Lanreotide Autogel in Acromegalic Patients (J Korean Endocr Soc 25:37-45, 2010)
