Non-invasive MR Demonstration of the Fistula between Pancreatic Pseudocyst and Portal Vein: A Case Report
- Affiliations
-
- 1Department of Radiology, School of Medicine, Catholic University of Daegu, Daegu, Korea. yhlee@cu.ac.kr
- KMID: 2099894
- DOI: http://doi.org/10.13104/jksmrm.2014.18.2.171
Abstract
- Pancreatic pseudocyst rupture into the portal vein is a very rare complication and only three reported cases were confirmed using MRI. We report the case of a 50-year-old man with fistula formation between the pseudocyst and the portal vein, confirmed noninvasively by MRI. T2-weighted MR images and magnetic resonance cholangiopancreatography showed fluid signal intensity within the portal, superior mesenteric, and splenic veins, and a direct communication between the pseudocyst and the portal vein.
Keyword
MeSH Terms
Figure
-

Fig. 1 Contrast enhanced CT. a. A 4 cm pseudocyst (asterisk) in the region of neck of the pancreas. b. Fluid density is seen within the thrombosed superior mesenteric (arrow) and splenic veins (arrowheads) without contrast enhancement. c. Fluid density is also seen within the main portal vein (arrow) and the right portal vein (arrowheads) is completely thrombosed. Cavernous transformation around the thrombosed portal vein.
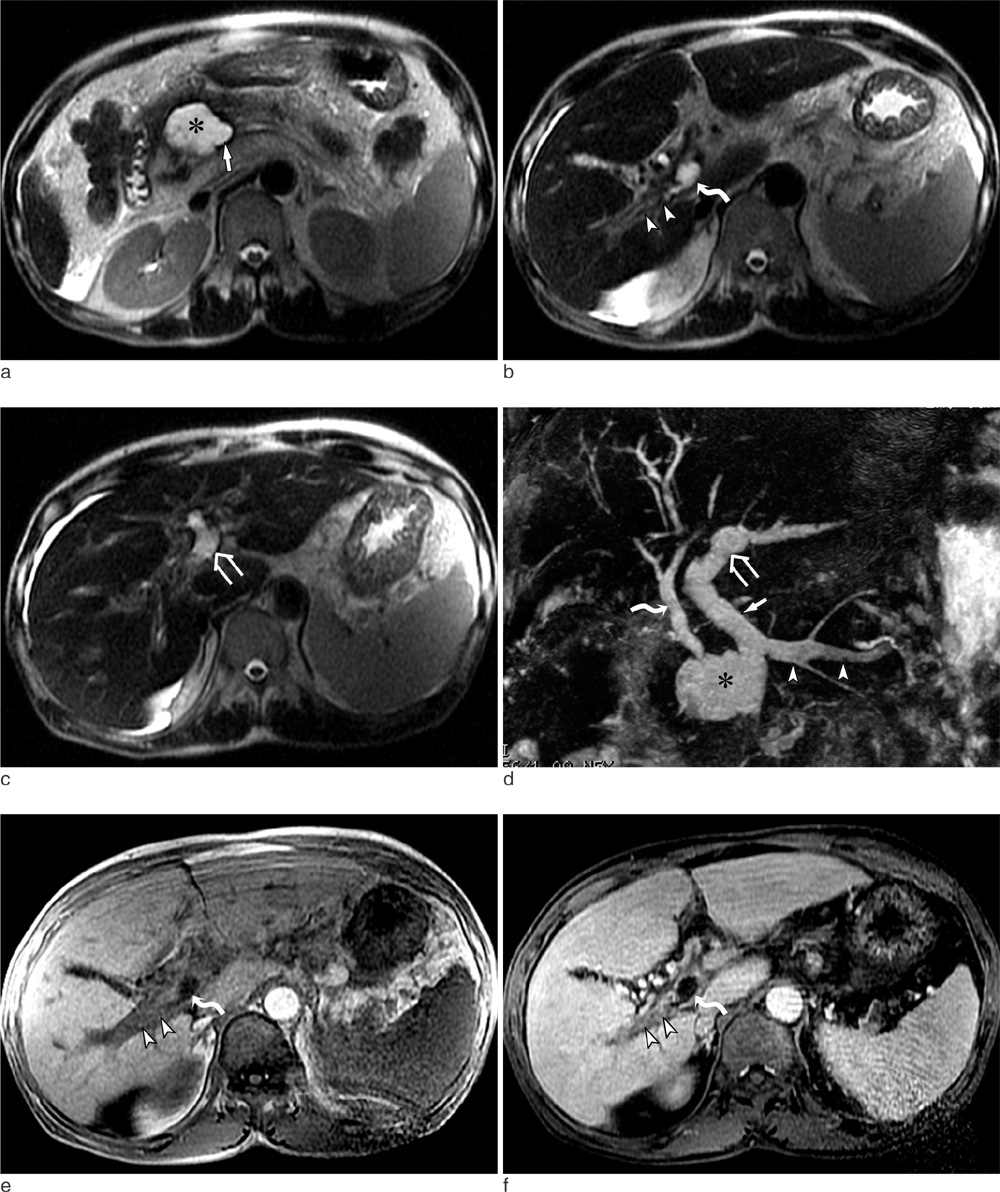
Fig. 2 a-c. Single-shot FSE T2-weighted images show a communication of the pseudocyst (asterisk) with the splenoportal confluence (arrow). Fluid signal intensity is seen within the main portal (curved arrow) and left portal (open arrow) veins. Right portal vein thrombosis (arrowheads) shows intermediate to low signal intensity. d. Coronal MIP MRCP image clearly demonstrates a direct communication of the pseudocyst (asterisk) with the splenoportal confluence. Fluid signal intensity is seen within the main portal (arrow), left portal (open arrow), and splenic (arrowheads) veins. Bile duct (curved arrow). e. T1-weighted SPGR image. Right portal vein thrombosis (arrowheads) shows intermediate signal intensity. Low signal intensity is seen within the main portal vein (curved arrow). f. Fat-saturated contrast-enhanced axial T1-weighted SPGR image. No contrast enhancement is seen in the right (arrowheads) and main portal vein (curved arrow).
Reference
-
1. Mortele KJ, Mergo PJ, Taylor HM, et al. Peripancreatic vascular abnormalities complicating acute pancreatitis: contrast-enhanced helical CT findings. Eur J Radiol. 2004; 52:67–72.2. Procacci C, Mansueto GC, Graziani R, et al. Spontaneous rupture of a pancreatic pseudocyst into the portal vein. Cardiovasc Intervent Radiol. 1995; 18:399–402.3. Riddell A, Jhaveri K, Haider M. Pseudocyst rupture into the portal vein diagnosed with MRI. Br J Radiol. 2005; 78:265–268.4. Yoon SE, Lee YH, Yoon KH, Choi CS, Kim HC, Chae KM. Spontaneous pancreatic pseudocyst-portal vein fistula presenting with pancreatic ascites: strength of MR cholangiopancreatography. Br J Radiol. 2008; 81:e13–e16.5. Dawson BC, Kasa D, Mazer MA. Pancreatic pseudocyst rupture into the portal vein. South Med J. 2009; 102:728–732.6. Dayal M, Sharmaa R, Madhusudhana KS, Gargb PK. MRI diagnosis of rupture of pancreatic pseudocyst into portal vein: case report and review of literature. Ann Gastroenterol. 2014; 27:173–176.7. Belli M, Jennings CM, Nakielny RA. Splenic and portal venous thrombosis: a vascular complication of pancreatic disease demonstrated on computed tomography. Clin Radiol. 1990; 41:13–16.8. Noh R, Kim HJ. A pancreatic pseudocyst-portal vein fistula closed by endoscopic pancreatic stent insertion. Gastrointest Endosc. 2010; 72:1103–1105.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pancreatic Pseudocyst-Portal Vein Fistula: Serial Imaging and Clinical Follow-up from Pseudocyst to Fistula
- A Case of Pancreatic Duct-Portal Vein Fistulae in Pancreatic Cancer
- Intrahepatic Bile Duct Dilatation Caused by Pancreatic Pseudocyst: A Case Report
- A Case of Cystoduodenal and Cystocolic Fistula Complicated in Pancreatic Pseudocyst
- A Gastric Hemorrhage through the Fistula between Stomach and Pancreatic Pseudocyst with Ruptured Splenic Artery Pseudoaneurysm : A Case Report
