Pancreatic Pseudocyst-Portal Vein Fistula: Serial Imaging and Clinical Follow-up from Pseudocyst to Fistula
- Affiliations
-
- 1Department of Radiology, Dankook University Hospital, Dankook University College of Medicine, Cheonan, Korea. jkn1303@dreamwiz.com
- KMID: 2161170
- DOI: http://doi.org/10.3348/jksr.2015.72.3.180
Abstract
- Pancreatic pseudocyst-portal vein fistula is an extremely rare complication of pancreatitis. Only 18 such cases have been previously reported in the medical literature. However, a serial process from pancreatic pseudocyst to fistula formation has not been described. The serial clinical and radiological findings in a 52-year-old chronic alcoholic male patient with fistula between pancreatic pseudocyst and main portal vein are presented.
MeSH Terms
Figure
-
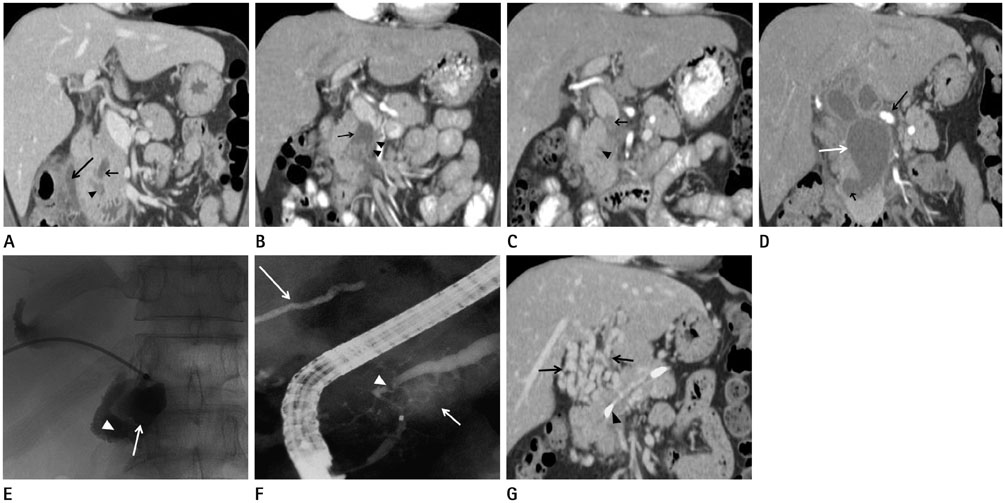
Fig. 1 Pancreatic pseudocyst-portal vein fistula in a 52-year-old chronic alcoholic male patient. A. Contrast-enhanced CT scan with coronal reformation shows a small cystic lesion (short arrow) in the pancreatic head and a few small fluid collections at pancreaticoduodenal groove (arrowhead) and periduodenal area (long arrow). B. Contrast-enhanced CT scan with coronal reformation shows increased size of the pseudocyst (arrow) in the pancreatic head with high attenuating debris or blood clot on dependent portion, compression of adjacent portal vein by the cystic lesion and short segmental thrombus in the proximal superior mesenteric vein (arrowheads). C. Contrast-enhanced abdominal CT scan with coronal reformation shows a very small pseudocyst (arrowhead) in the head of pancreas and thrombus expansion into the distal main portal vein (arrow). D. Contrast-enhanced CT scan with coronal reformation shows low attenuating pseudocyst (short black arrow) in the pancreatic head adjacent to the portal vein (white arrow) and surrounding periportal collateral vessels (long black arrow). E. Percutaneous transhepatic portography shows contrast filled dilated main portal vein (arrow) and extravasation of contrast material into the pseudocyst (arrowhead). F. Endoscopic retrograde pancreatography shows dilatation of main pancreatic duct and a stricture (arrowhead) communicating with contrast filled pseudocyst (arrow). Glue embolization state of right portal vein is shown at superior side (long arrow). G. Contrast-enhanced CT scan with coronal reformation shows extensive periportal collateral vessels (arrows), obliteration of main portal vein, disappeared pseudocyst in the pancreatic head and stent (arrowhead) in main pancreatic duct.
Reference
-
1. Aghdassi A, Mayerle J, Kraft M, Sielenkämper AW, Heidecke CD, Lerch MM. Diagnosis and treatment of pancreatic pseudocysts in chronic pancreatitis. Pancreas. 2008; 36:105–112.2. Hammar AM, Sand J, Lumio J, Hirn M, Honkonen S, Tuominen L, et al. Pancreatic pseudocystportal vein fistula manifests as residivating oligoarthritis, subcutaneous, bursal and osseal necrosis: a case report and review of literature. Hepatogastroenterology. 2002; 49:273–278.3. Yamamoto T, Hayakawa K, Kawakami S, Nishimura K, Katsuma Y, Hayashi N, et al. Rupture of a pancreatic pseudocyst into the portal venous system. Abdom Imaging. 1999; 24:494–496.4. Bradley EL, Clements JL Jr, Gonzalez AC. The natural history of pancreatic pseudocysts: a unified concept of management. Am J Surg. 1979; 137:135–141.5. Kaman L, Behera A, Singh R, Katariya RN. Internal pancreatic fistulas with pancreatic ascites and pancreatic pleural effusions: recognition and management. ANZ J Surg. 2001; 71:221–225.6. Lee SH, Bodensteiner D, Eisman S, Dixon AY, McGregor DH. Chronic relapsing pancreatitis with pseudocyst erosion into the portal vein and disseminated fat necrosis. Am J Gastroenterol. 1985; 80:452–458.7. Skarsgard ED, Ellison E, Quenville N. Spontaneous rupture of a pancreatic pseudocyst into the portal vein. Can J Surg. 1995; 38:459–463.8. Van Steenbergen W, Ponette E. Pancreaticoportal fistula: a rare complication of chronic pancreatitis. Gastrointest Radiol. 1990; 15:299–300.9. Yoon SE, Lee YH, Yoon KH, Choi CS, Kim HC, Chae KM. Spontaneous pancreatic pseudocyst-portal vein fistula presenting with pancreatic ascites: strength of MR cholangiopancreatography. Br J Radiol. 2008; 81:e13–e16.10. Brown A, Malden E, Kugelmas M, Kortz E. Diagnosis of pancreatic duct-portal vein fistula; a case report and review of the literature. J Radiol Case Rep. 2014; 8:31–38.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Non-invasive MR Demonstration of the Fistula between Pancreatic Pseudocyst and Portal Vein: A Case Report
- Intrahepatic Bile Duct Dilatation Caused by Pancreatic Pseudocyst: A Case Report
- A Case of Cystoduodenal and Cystocolic Fistula Complicated in Pancreatic Pseudocyst
- Mediastinal pancreatic pseudocyst naturally drained by esophageal fistula
- A Gastric Hemorrhage through the Fistula between Stomach and Pancreatic Pseudocyst with Ruptured Splenic Artery Pseudoaneurysm : A Case Report
