Towards Routine Clinical Use of Radial Stack-of-Stars 3D Gradient-Echo Sequences for Reducing Motion Sensitivity
- Affiliations
-
- 1Bernard and Irene Schwartz Center for Biomedical Imaging, New York University School of Medicine, New York, USA. Tobias.Block@nyumc.org
- 2Pattern Recognition Lab, University of Erlangen-Nuremberg, Erlangen, Germany.
- 3Siemens Medical Solutions Inc, New York, USA.
- 4Siemens AG Healthcare MR, Erlangen, Germany.
- KMID: 2099886
- DOI: http://doi.org/10.13104/jksmrm.2014.18.2.87
Abstract
- PURPOSE
To describe how a robust implementation of a radial 3D gradient-echo sequence with stack-of-stars sampling can be achieved, to review the imaging properties of radial acquisitions, and to share the experience from more than 5000 clinical patient scans.
MATERIALS AND METHODS
A radial stack-of-stars sequence was implemented and installed on 9 clinical MR systems operating at 1.5 and 3 Tesla. Protocols were designed for various applications in which motion artifacts frequently pose a problem with conventional Cartesian techniques. Radial scans were added to routine examinations without selection of specific patient cohorts.
RESULTS
Radial acquisitions show significantly lower sensitivity to motion and allow examinations during free breathing. Elimination of breath-holding reduces failure rates for non-compliant patients and enables imaging at higher resolution. Residual artifacts appear as streaks, which are easy to identify and rarely obscure diagnostic information. The improved robustness comes at the expense of longer scan durations, the requirement for fat suppression, and the nonexistence of a time-to-center value. Care needs to be taken during the configuration of receive coils.
CONCLUSION
Routine clinical use of radial stack-of-stars sequences is feasible with current MR systems and may serve as substitute for conventional fat-suppressed T1-weighted protocols in applications where motion is likely to degrade the image quality.
Keyword
MeSH Terms
Figure
-

Fig. 1 (a) "Stack-of-stars" trajectory, which acquires the kx-ky plane along radial spokes and the kz direction with Cartesian sampling. The angle of the radial spokes can be ordered (b) using an equidistant scheme or (c) using the golden-angle scheme. Numbers indicate the temporal order of the acquisition.

Fig. 2 Basic pulse sequence diagram for one TR repetition cycle, starting with a RF excitation pulse (a), which is used either without or with slab-selection gradient (b). Gradient pulse (c) combines slab-selection rewinding and Cartesian phase encoding along the SLICE axis. Gradient pulses (d) act as dephasing, (e) readout, and (g) spoiling gradients in the READ-PHASE plane. Gradients (d, e, g) are played simultaneously in the READ and PHASE direction with amplitudes modulated according to Eq. (1), resulting in radial k-space traversal. The signal is recorded using an ADC event (f) during the flat-top time of the readout gradients (e). Gradient pulse (h) spoils residual magnetization along the SLICE axis. Gray color indicates that gradient amplitudes are changing per repetition.

Fig. 3 Free-breathing abdominal exam using (a) conventional Cartesian sampling and (b) radial sampling (with otherwise identical sequence parameters and matching acquisition time). While the Cartesian scan suffers from strong "ghosting" artifacts, the radial acquisition provides diagnostic image quality.

Fig. 4 Scan with reduced FOV size using (a) Cartesian sampling and (b) radial sampling. Due to the large object extent, aliasing occurs with Cartesian sampling along the phase-encoding direction. Because readout oversampling can be applied in both directions, aliasing does not appear with radial sampling.
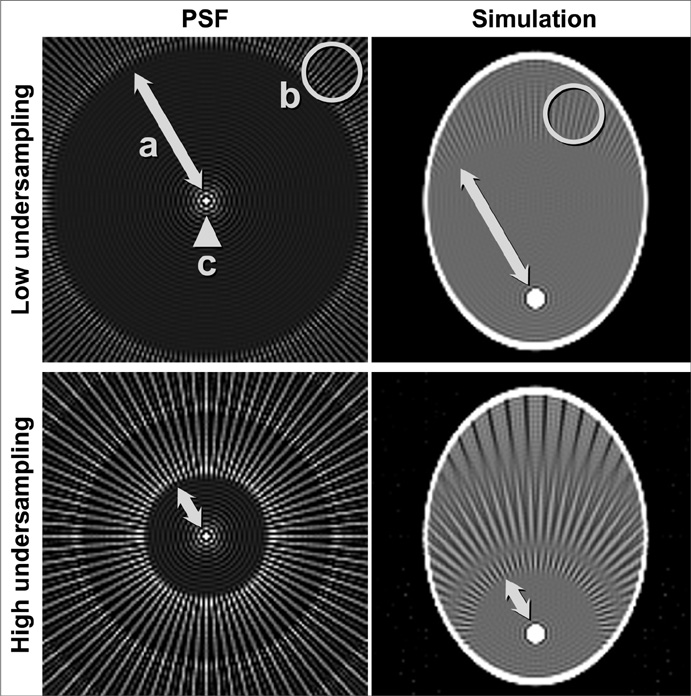
Fig. 5 (Left) Radial point-spread-function and (right) exemplary imaging simulation for (top) mild and (bottom) strong undersampling. The PSF has a central peak (c), which reflects the obtained spatial resolution and whose width is independent of the undersampling. It is surrounded by a dense disc with minor circular Gibbs ringing. Beyond the Nyquist radius (a), which depends on the number of acquired spokes, it shows radially propagating streak patterns (b). The high-intensity circle of the simulation object therefore leads to streaks in the reconstructed image at Nyquist distance. A streak-free image is obtained if the largest object diameter is smaller than the Nyquist radius.

Fig. 6 (a) Without correction of gradient delays, radial scans suffer from intensity modulations and streaks around the object. (b) Corrected radial scan after applying the described adaptive calibration approach.

Fig. 7 (Top) Off-resonant fat signal leads to the well-known chemical-shift artifact along the readout direction for Cartesian trajectories. (Middle) Due to the varying readout orientation, the chemical-shift effect translates into signal blurring for radial sampling. (Bottom) The effect can be avoided by using radial sampling with fat-suppression.

Fig. 8 (a) Severe streak artifacts appear in the thorax (arrows), which are caused by an improperly selected coil element with main sensitivity localization in the pelvic area (circle). (b) After disabling the coil, the streak artifacts disappear with negligible loss of the overall signal intensity in the region-of-interest.

Fig. 9 (a, c) Cartesian 3D GRE exam of the liver in patients unable to suspend respiration, compared to (b, d) examination during free breathing using the radial sequence. A lesion in the spleen (arrow in b) is only visible on the radial exam. An enlarged lymph node (arrow in d) is clearly identified on the radial exam but difficult to appreciate on the Cartesian exam.

Fig. 10 (a, c) The achievable resolution with Cartesian scans is limited by the typical breath-hold capacity of less than 20 sec. (b, d) Radial acquisition during free shallow breathing enables to obtain significantly higher spatial resolution. In the example of late-phase exam after injection of EOVIST, it provides much sharper depiction of the biliary duct (arrows).
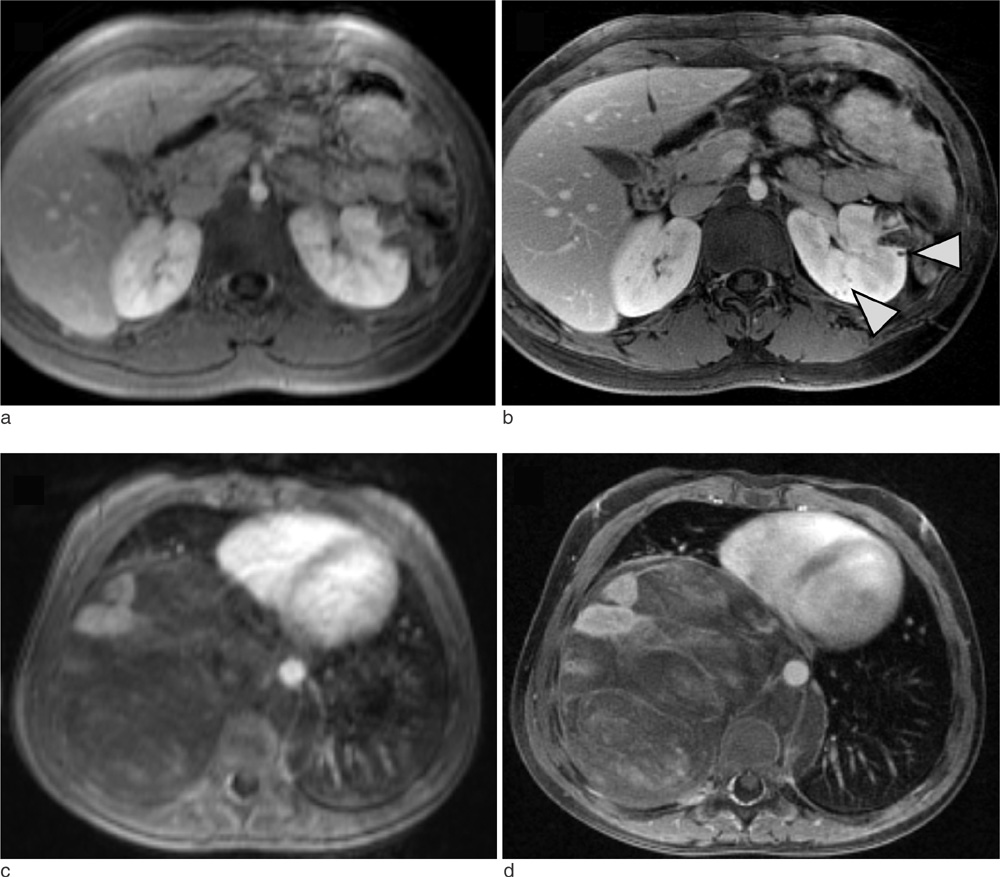
Fig. 11 Pediatric abdominopelvic exams are degraded by respiration artifacts when performed with conventional sequences during sedation (a, c), which limit the effective resolution. Significantly improved image quality is achieved with the radial sequence (b, d). In the case of a patient with Tuberous Sclerosis (top), the radial sequence reveals small cysts in the kidney (arrows).

Fig. 12 Brain exam of a 4-week-old active patient using (a) 2D TSE, (b) MP-RAGE, (c) 2D FLASH, and (d) the radial sequence. While all Cartesian sequences were affected by a certain level of motion artifacts, the radial sequence provided acceptable diagnostic image quality.

Fig. 13 Imaging of the neck (a, b) and upper chest (c, d) using a conventional 2D TSE sequence (a, c) and the radial sequence (b, d). Due to strong motion and flow artifacts, a mass in the thyroid gland is not visible on the 2D TSE exam but appreciated on the radial scan (arrow in b). Evaluation of the sternum in a patient complaining of pain was not possible on the 2D TSE scan (c), but unproblematic with the radial sequence (d).

Fig. 14 Multi-planar reconstructions of a radial neck scan with 1.0 mm isotropic resolution, which are unaffected from swallowing or respiration artifacts and which can be used as replacement for separate 2D TSE acquisitions in these orientations. Of note is a failure of spectral fat saturation in the back of the neck, which is a common observation in the proximity of skin folds. Furthermore, the outer slices show slight aliasing along kz, caused by imperfections of the slab-selective excitation pulse. Both effects are not related to the radial scheme.
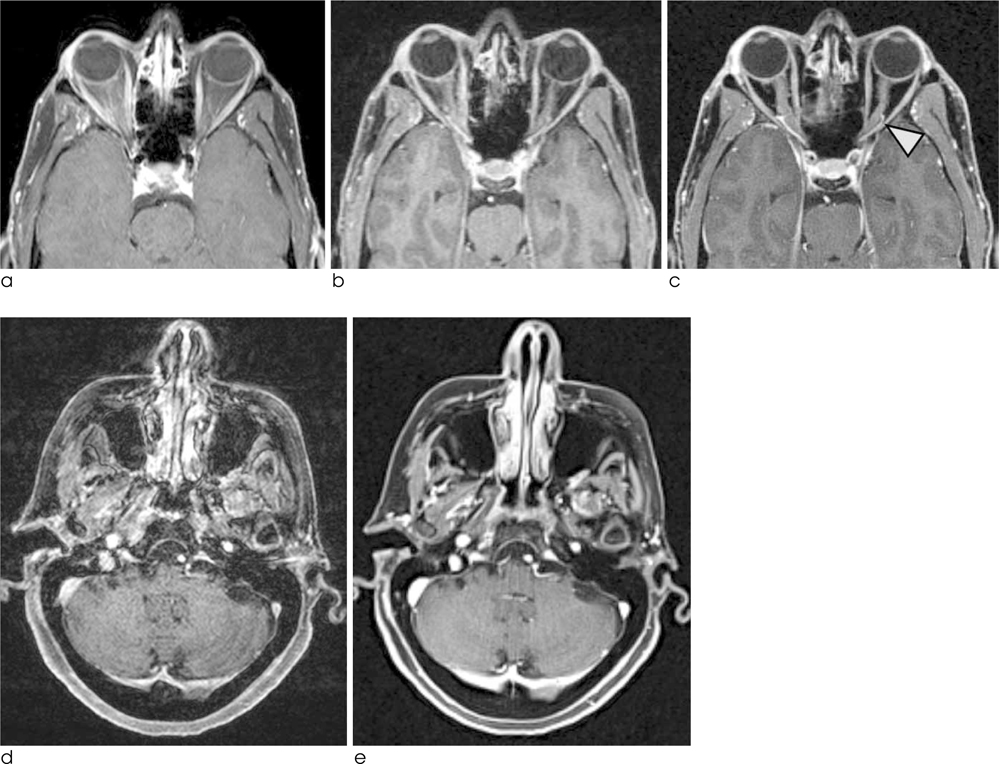
Fig. 15 (Top) Imaging of the orbits using (a) 2D TSE, (b) MP-RAGE, and (c) the radial sequence. Both Cartesian scans are affected by motion artifacts that limit the clarity of the optic nerves. The radial sequence provides sharp visualization of the optic nerves and surrounding vessels (arrow). (Bottom) Imaging of the full brain using (d) MR-RAGE and (e) the radial sequence, which shows significantly lower motion artifacts and higher image clarity.

Fig. 16 Spine imaging in patients with metastasis using (a, c) conventional 2D TSE sequences without fat suppression and (b, d) the radial sequence. The radial sequence shows clear contrast enhancement of the metastasis (arrows), while the enhancement is more difficult to see on the TSE scans because of low contrast difference to normal bone marrow and because of ghosting artifacts arising from blood flow and organ movement.
Cited by 1 articles
-
Rapid Imaging: Recent Advances in Abdominal MRI for Reducing Acquisition Time and Its Clinical Applications
Jeong Hee Yoon, Marcel Dominik Nickel, Johannes M. Peeters, Jeong Min Lee
Korean J Radiol. 2019;20(12):1597-1615. doi: 10.3348/kjr.2018.0931.
Reference
-
1. Kumar A, Welti D, Ernst RR. NMR Fourier zeugmatography. J Magn Reson. 1975; 18:69–83.2. Meyer CH, Hu BS, Nishimura DG, Macovski A. Fast spiral coronary artery imaging. Magn Reson Med. 1992; 28:202–213.3. Crémillieux Y, Briguet A, Deguin A. Projection-reconstruction methods: fast imaging sequences and data processing. Magn Reson Med. 1994; 32:23–32.4. Mistretta CA, Wieben O, Velikina J, et al. Highly constrained backprojection for time-resolved MRI. Magn Reson Med. 2006; 55:30–40.5. Du J, Carroll TJ, Brodsky E, et al. Contrast-enhanced peripheral magnetic resonance angiography using time-resolved vastly undersampled isotropic projection reconstruction. J Magn Reson Imaging. 2004; 20:894–900.6. Lustig M, Donoho D, Pauly JM. Sparse MRI: the application of compressed sensing for rapid MR imaging. Magn Reson Med. 2007; 58:1182–1195.7. Pipe JG. Motion correction with PROPELLER MRI: application to head motion and free-breathing cardiac imaging. Magn Reson Med. 1999; 42:963–969.8. Nishimura DG, Jackson JI, Pauly JM. On the nature and reduction of the displacement artifact in flow images. Magn Reson Med. 1991; 22:481–492.9. Chandarana H, Block KT, Rosenkrantz AB, et al. Free-breathing radial 3D fat-suppressed T1-weighted gradient echo sequence: a viable alternative for contrast-enhanced liver imaging in patients unable to suspend respiration. Invest Radiol. 2011; 46:648–653.10. Azevedo RM, de Campos RO, Ramalho M, Héredia V, Dale BM, Semelka RC. Free-breathing 3D T1-weighted gradient-echo sequence with radial data sampling in abdominal MRI: preliminary observations. AJR Am J Roentgenol. 2011; 197:650–657.11. Chandarana H, Block KT, Winfeld MJ, et al. Free-breathing contrast-enhanced T1-weighted gradient-echo imaging with radial k-space sampling for paediatric abdominopelvic MRI. Eur Radiol. 2014; 24:320–326.12. Wu X, Raz E, Block KT, et al. Contrast-enhanced radial 3D fat-suppressed T1-weighted gradient-echo (Radial-VIBE) sequence: a viable and potentially superior alternative to conventional fat-suppressed contrast-enhanced T1-weighted studies of the head and neck. Am J Roentgenol. 2014; in press.13. Chandarana H, Heacock L, Rakheja R, et al. Pulmonary nodules in patients with primary malignancy: comparison of hybrid PET/MR and PET/CT imaging. Radiology. 2013; 268:874–881.14. Bamrungchart S, Tantaway EM, Midia EC, et al. Free breathing three-dimensional gradient echo-sequence with radial data sampling (radial 3D-GRE) examination of the pancreas: Comparison with standard 3D-GRE volumetric interpolated breathhold examination (VIBE). J Magn Reson Imaging. 2013; 38:1572–1577.15. Bernstein MA, King KF, Xiaohong JZ. Handbook of MRI pulse sequences. Waltham: Elsevier Academic Press;2004.16. Winkelmann S, Schaeffter T, Koehler T, Eggers H, Doessel O. An optimal radial profile order based on the Golden Ratio for time-resolved MRI. IEEE Trans Med Imaging. 2007; 26:68–76.17. Block KT. Advanced methods for radial data sampling in magnetic resonance imaging. SUB University of Goettingen;2008. 09. 16. Accessed January 9, 2014. http://webdoc.sub.gwdg.de/diss/2008/block/block.pdf.18. Ramachandran GN, Lakshminarayanan AV. Three-dimensional reconstruction from radiographs and electron micrographs: application of convolutions instead of Fourier transforms. Proc Natl Acad Sci USA. 1971; 68:2236–2240.19. Beatty PJ, Nishimura DG, Pauly JM. Rapid gridding reconstruction with a minimal oversampling ratio. IEEE Trans Med Imaging. 2005; 24:799–808.20. Jackson JI, Meyer CH, Nishimura DG, Macovski A. Selection of a convolution function for Fourier inversion using gridding. IEEE Trans Med Imaging. 1991; 10:473–478.21. Peters DC, Korosec FR, Grist TM, et al. Undersampled projection reconstruction applied to MR angiography. Magn Reson Med. 2000; 43:91–101.22. Alley MT, Glover GH, Pelc NJ. Gradient characterization using a Fourier-transform technique. Magn Reson Med. 1998; 39:581–587.23. Peters DC, Derbyshire JA, McVeigh ER. Centering the projection reconstruction trajectory. Magn Reson Med. 2003; 50:1–6.24. Block KT, Uecker M. Simple method for adaptive gradient-delay compensation in radial MRI. Proceedings of the 19th scientific meeting, International Society for Magnetic Resonance in Medicine 2011. Montréal. p. 2816.25. Brodsky EK, Holmes JH, Yu H, Reeder SB. Generalized k-space decomposition with chemical shift correction for non-Cartesian water-fat imaging. Magn Reson Med. 2008; 59:1151–1164.26. Xue Y, Yu J, Kang HS, Englander S, Rosen MA, Song HK. Automatic coil selection for streak artifact reduction in radial MRI. Magn Reson Med. 2012; 67:470–476.27. Pruessmann KP, Weiger M, Börnert P, Boesiger P. Advances in sensitivity encoding with arbitrary k-space trajectories. Magn Reson Med. 2001; 46:638–651.28. Seiberlich N, Breuer FA, Ehses P, et al. Using the GRAPPA operator and the generalized sampling theorem to reconstruct undersampled non-Cartesian data. Magn Reson Med. 2009; 61:705–715.29. Harvey JA, Hendrick RE, Coll JM, Nicholson BT, Burkholder BT, Cohen MA. Breast MR imaging artifacts: how to recognize and fix them. Radiographics. 2007; 27:S131–S145.30. Song HK, Dougherty L. Dynamic MRI with projection reconstruction and KWIC processing for simultaneous high spatial and temporal resolution. Magn Reson Med. 2004; 52:815–824.31. Altbach MI, Bilgin A, Li Z, Clarkson EW, Trouard TP, Gmitro AF. Processing of radial fast spin-echo data for obtaining T2 estimates from a single k-space data set. Magn Reson Med. 2005; 54:549–559.32. Feng L, Grimm R, Block KT, et al. Golden-angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magn Reson Med. 2013; Epub ahead of print, 10.1002/mrm.24980.33. Chandarana H, Feng L, Block KT, et al. Free-breathing contrast-enhanced multiphase MRI of the liver using a combination of compressed sensing, parallel imaging and golden-angle radial sampling. Invest Radiol. 2013; 48:10–16.34. Grimm R, Block KT, Hutter J, et al. Self-gating reconstructions of motion and perfusion for free-breathing T1-weighted DCE-MRI of the thorax using 3D stack-of-stars GRE imaging. Proceedings of the 20th scientific meeting, International Society for Magnetic Resonance in Medicine 2012. Melbourne: p. 3814.35. Lin W, Guo J, Rosen MA, Song HK. Respiratory motion-compensated radial dynamic contrast-enhanced (DCE)-MRI of chest and abdominal lesions. Magn Reson Med. 2008; 60:1135–1146.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Gradient Optimized Gradient-Echo Gradient Moment Nulling Sequences for Flow Compensation of Brain mages
- A Unified Gradient Shape on the Slice-Selection Axis for Flow Compensation
- Advanced Methods in Dynamic Contrast Enhanced Arterial Phase Imaging of the Liver
- T1-weighted MR Imaging of the Neonatal Brain at 3.0 Tesla: Comparison of Spin Echo, Fast Inversion Recovery, and Magnetization-prepared Three Dimensional Gradient Echo Techniques
- Single-Slab 3D Fast Spin Echo Imaging: T1 -Contrast Perspective
