J Korean Surg Soc.
2011 Nov;81(5):355-359. 10.4174/jkss.2011.81.5.355.
Robotic pylorus preserving pancreaticoduodenectomy with mini-laparotomy reconstruction in patient with ampullary adenoma
- Affiliations
-
- 1Department of Surgery, Yonsei University College of Medicine, Institute of Gastroenterology, Yonsei University Health System, Seoul, Korea. cmkang@yuhs.ac
- 2Department of Surgery, Wonju Christian Hospital, Yonsei University Wonju College of Medicine, Wonju, Korea.
- KMID: 2096691
- DOI: http://doi.org/10.4174/jkss.2011.81.5.355
Abstract
- Robotic surgical system provides many unique advantages which might compensate the limitations of usual laparoscopic surgery. By using robotic surgical system, we performed robot-assisted laparoscopic pancreaticoduodenectomy (PD). A Sixty-two year old female patient with an ampullary mass underwent robot assisted PD due to imcomplete treatment of endoscopic ampullectomy. The removal of specimen and reconstruction were performed through small upper midline skin incision. Robot working time was about 8 hours, and blood loss was about 800 ml without blood transfusion. She returned to an oral diet on postoperative day 3. Grade B pancreatic leak was noted during the postoperative period, but was successfully managed by conservative management alone. We successfully performed da Vinci-assisted laparoscopic PD, and robot surgical system provided three-dimensional stable visualization and wrist-like motion of instrument facilitated complex operative procedures. More experiences are necessary to address real role of robot in far advanced laparoscopic pancreatic surgery.
Keyword
MeSH Terms
Figure
-
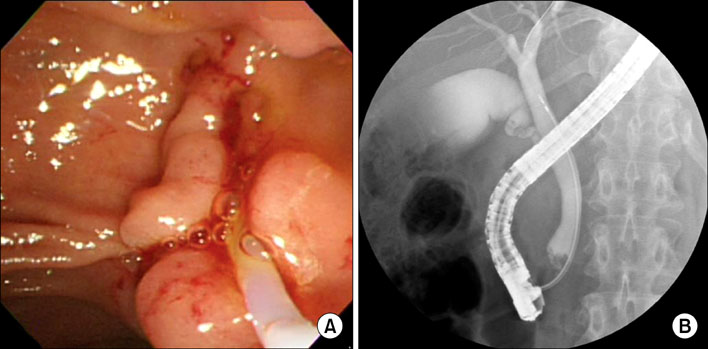
Fig. 1 (A) Endoscopic retrograde cholangiopancreatography showed polypoid mass protruding out of the orifice of common bile duct (CBD). (B) On cholangiogram, filling defect was noted at distal CBD area.
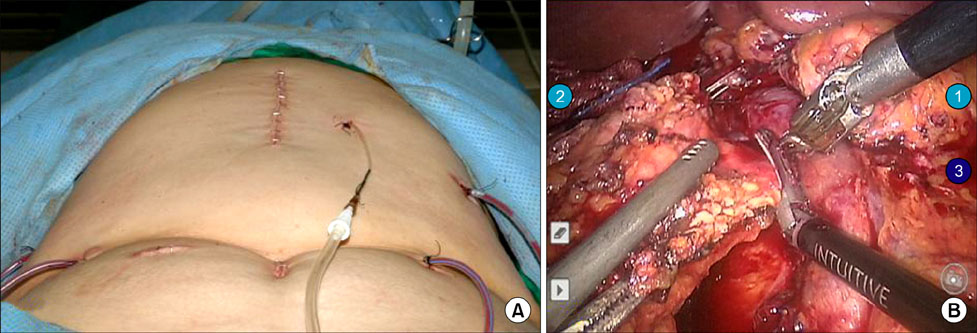
Fig. 2 (A) Port sites and postoperative wound, which was much smaller than that of conventional open pancreaticoduodenectomy. (B) Three-dimensional surgical field, stable portal vein retraction by another robotic arm without tremor helped the surgeon fully focus on sharp dissection of the uncinate process from retroperitoneal reflection.
Reference
-
1. Crile G Jr. The advantages of bypass operations over radical pancreatoduodenectomy in the treatment of pancreatic carcinoma. Surg Gynecol Obstet. 1970. 130:1049–1053.2. Cameron JL, Riall TS, Coleman J, Belcher KA. One thousand consecutive pancreaticoduodenectomies. Ann Surg. 2006. 244:10–15.3. Gagner M, Pomp A. Laparoscopic pylorus-preserving pancreatoduodenectomy. Surg Endosc. 1994. 8:408–410.4. Park A, Schwartz R, Tandan V, Anvari M. Laparoscopic pancreatic surgery. Am J Surg. 1999. 177:158–163.5. Kendrick ML, Cusati D. Total laparoscopic pancreaticoduodenectomy: feasibility and outcome in an early experience. Arch Surg. 2010. 145:19–23.6. Kim MC, Jung GJ, Kim HH. Learning curve of laparoscopy -assisted distal gastrectomy with systemic lymphadenectomy for early gastric cancer. World J Gastroenterol. 2005. 11:7508–7511.7. Kang CM, Chi HS, Kim JY, Choi GH, Kim KS, Choi JS, et al. A case of robot-assisted excision of choledochal cyst, hepaticojejunostomy, and extracorporeal Roux-en-y anastomosis using the da Vinci surgical system. Surg Laparosc Endosc Percutan Tech. 2007. 17:538–541.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Robotic transduodenal ampullectomy: Case report and review of the literature
- Pylorus preserving pancreaticoduodenectomy; short term result
- Surgery for Ampulla of Vater Adenoma
- Endoscopic Management of Afferent Loop Syndrome after a Pylorus Preserving Pancreatoduodenecotomy Presenting with Obstructive Jaundice and Ascending Cholangitis
- A Case of Successful Embolization with Superselection by Endoscopic Hemoclipping for Pseudoaneurysmal Bleeding in a Patient with Pylorus Preserving Pancreaticoduodenectomy
