Dialysis Catheter-Related Superior Vena Cava Syndrome with Patent Vena Cava: Long Term Efficacy of Unilateral Viatorr Stent-Graft Avoiding Catheter Manipulation
- Affiliations
-
- 1Unit of Interventional Radiology - Radiology Department, IRCCS Policlinico San Matteo Foundation, Pavia 27100, Italy. p.quaretti@smatteo.pv.it
- 2Nephrology and Dialysis, IRCCS Fondazione Salvatore Maugeri, Pavia 27100, Italy.
- 3Department of General Surgery, IRCCS Policlinico San Matteo Foundation, Pavia 27100, Italy.
- KMID: 2078646
- DOI: http://doi.org/10.3348/kjr.2014.15.3.364
Abstract
- Central venous catheters are the most frequent causes of benign central vein stenosis. We report the case of a 79-year-old woman on hemodialysis through a twin catheter in the right internal jugular vein, presenting with superior vena cava (SVC) syndrome with patent SVC. The clinically driven endovascular therapy was conducted to treat the venous syndrome with a unilateral left brachiocephalic stent-graft without manipulation of the well-functioning catheter. The follow-up was uneventful until death 94 months later.
Keyword
MeSH Terms
Figure
-
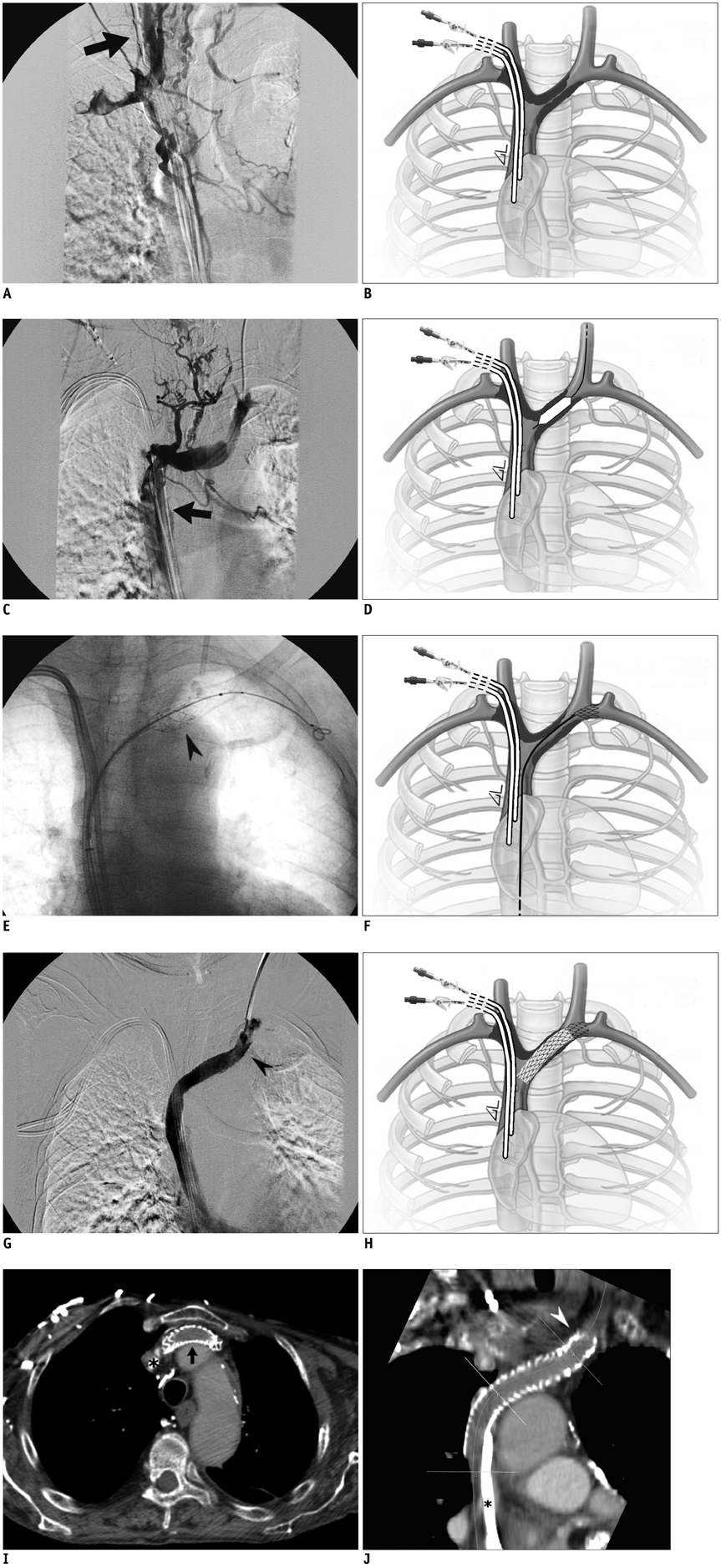
Fig. 1 Angiographic and schematic illustration of procedure. A. Diagnostic angiography through distal right internal jugular vein injection shows occlusion of right brachiocephalic vein around twin catheter and inverted flow in internal jugular vein (arrow). B. Schematic drawing illustrates initial situation with pericatheter thrombosis involving right internal jugular vein, right subclavian vein and right brachiocephalic vein around well functioning twin catheter. C. Venography from left internal jugular vein reveals critical stenosis of distal left brachiocephalic vein with proximal collateral pathways and patent superior vena cava (arrow). D. Draw illustrates 8 mm predilation of left brachiocephalic lesion performed from left internal jugular vein access subsequently followed by immediate and complete elastic recoil. E. Leading bare end of stent-graft (arrowhead) is open after retrieval of 10-Fr introducer at fluoroscopy snap shot during transfemoral stent-graft releasing. F. Schematic drawing shows free-flow leading end of stent-graft in front of opening to left internal jugular vein. G. Final venography from left internal jugular vein introducer shows direct free flow in right atrium through leading bare end (arrowhead) of Viatorr stent-graft. H. Draw represents final situation with expanded stent-graft permitting flow from left internal jugular vein and left brachiocephalic vein. I. Axial contrast-enhanced multidetector computed tomography performed at 60 months for breast cancer follow-up showing stent-graft (arrow) patency and twin catheter (star). J. Curved multi-planar reconstruction through longitudinal axis of Viatorr stent-graft confirms stent patency (arrowhead) and twin catheter (star) in site.
Reference
-
1. Agarwal AK. Central vein stenosis. Am J Kidney Dis. 2013; 61:1001–1015.2. Riutta JC, Cheville AL, Trerotola SO. SVC syndrome with a patent SVC: treatment of internal jugular venous occlusion after surgical and radiation therapy of esophageal cancer. J Vasc Interv Radiol. 2005; 16:727–731.3. III. NKF-K/DOQI Clinical Practice Guidelines for Vascular Access: update 2000. Am J Kidney Dis. 2001; 37:1 Suppl 1. S137–S181.4. Anaya-Ayala JE, Smolock CJ, Colvard BD, Naoum JJ, Bismuth J, Lumsden AB, et al. Efficacy of covered stent placement for central venous occlusive disease in hemodialysis patients. J Vasc Surg. 2011; 54:754–759.5. Kundu S, Modabber M, You JM, Tam P, Nagai G, Ting R. Use of PTFE stent grafts for hemodialysis-related central venous occlusions: intermediate-term results. Cardiovasc Intervent Radiol. 2011; 34:949–957.6. Verstandig AG, Berelowitz D, Zaghal I, Goldin I, Olsha O, Shamieh B, et al. Stent grafts for central venous occlusive disease in patients with ipsilateral hemodialysis access. J Vasc Interv Radiol. 2013; 24:1280–1287. quiz 1288.7. Jones RG, Willis AP, Jones C, McCafferty IJ, Riley PL. Long-term results of stent-graft placement to treat central venous stenosis and occlusion in hemodialysis patients with arteriovenous fistulas. J Vasc Interv Radiol. 2011; 22:1240–1245.8. Isfort P, Penzkofer T, Goerg F, Mahnken AH. Stenting of the superior vena cava and left brachiocephalic vein with preserving the central venous catheter in situ. Korean J Radiol. 2011; 12:629–633.9. Stockx L, Raat H, Donck J, Wilms G, Marchal G. Repositioning and leaving in situ the central venous catheter during percutaneous treatment of associated superior vena cava syndrome: a report of eight cases. Cardiovasc Intervent Radiol. 1999; 22:224–226.10. García-Pagán JC, Caca K, Bureau C, Laleman W, Appenrodt B, Luca A, et al. Early use of TIPS in patients with cirrhosis and variceal bleeding. N Engl J Med. 2010; 362:2370–2379.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Superior vena cava syndrome secondary to hickman catheter in the advanced cervical cancer patient treated with concurrent chemoradiotherapy: A case report
- A Case of Superior Vena Cava Syndrome
- Successful Treatment of Malignant Superior Vena Cava Syndrome Using a Stent-Graft
- Bypass of Superior Vena Cava with Spiral Vein Graft
- A Fatal Case of Acute Superior Vena Cava Syndrome and Mediastinal Hematoma Following Insertion of the Internal Jugular Catheter for Hemodialysis
