Successful Treatment of Malignant Superior Vena Cava Syndrome Using a Stent-Graft
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul 138-736, Korea.
- 2Department of Radiology, Soonchunhyang University Bucheon Hospital, Bucheon 420-767, Korea. radpsh@schmc.ac.kr
- KMID: 1245387
- DOI: http://doi.org/10.3348/kjr.2012.13.2.227
Abstract
- We report successful outcomes after endovascular placement of a stent graft in a 74- and a 77-year-old men, both of whom had malignant superior vena cava syndrome caused by squamous cell carcinoma. In each patient, successful palliation of the malignant superior vena cava syndrome was achieved by placement of a stent graft. No procedure-related complications were observed. The patients were asymptomatic until their deaths, seven and 14 months after stent graft placement, respectively.
Keyword
MeSH Terms
Figure
-
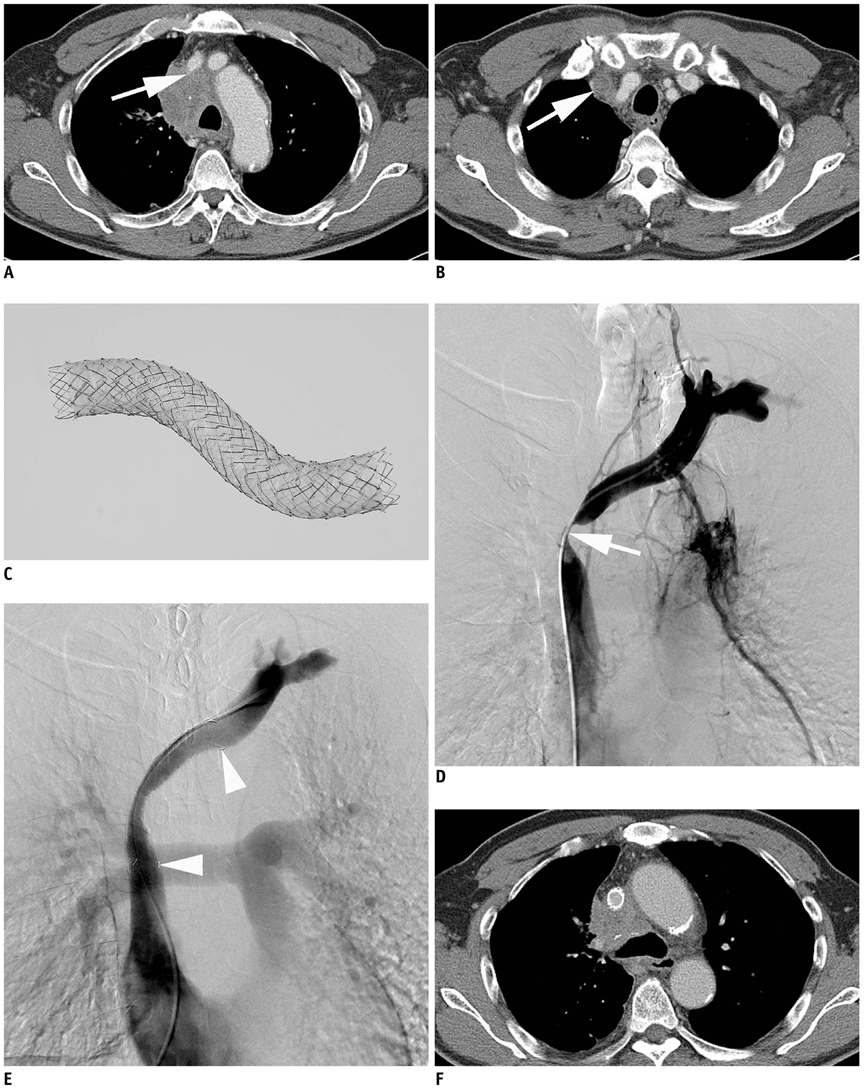
Fig. 1 Seventyfour-year-old man with malignant superior vena cava syndrome due to squamous cell carcinoma. A. Contrast-enhanced axial CT image shows central mass with mediastinal lymphadenopathy and left brachiocephalic venous obstruction (arrow). B. Axial CT image at upper level of A shows right brachiocephalic venous thrombosis (arrow). C. Partially expanded polytetrafluoroethylene-covered stent-graft used in these cases. D. Left brachiocephalic venography shows obstruction of confluence and proximal superior vena cava (arrow). E. Venography after stent-graft placement (14 mm × 8 cm) (arrowheads) shows fluent passage of contrast medium via stent. F. Contrast enhanced axial CT image obtained 11 months after stent-graft placement shows patent stent-graft.
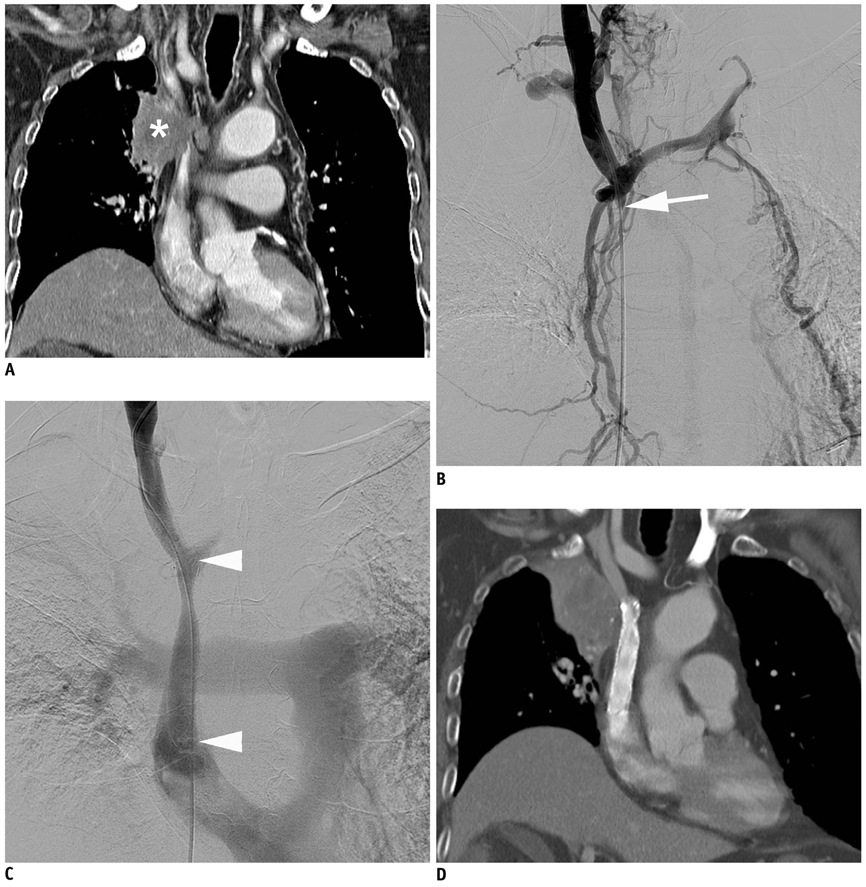
Fig. 2 Seventyseven-year-old man with malignant superior vena cava syndrome due to squamous cell carcinoma. A. Contrast-enhanced coronal CT image shows superior vena cava obstruction caused by central lung mass (asterisk). B. Right brachiocephalic venography shows obstruction of proximal superior vena cava (arrow) with collaterals. C. Venography after stent-graft placement (14 mm × 8 cm) (arrowheads) shows fluent passage of contrast medium via stent. D. Contrast-enhanced coronal CT image obtained four months after stent-graft placement shows patent stent-graft.
Reference
-
1. Rowell NP, Gleeson FV. Steroids, radiotherapy, chemotherapy and stents for superior vena caval obstruction in carcinoma of the bronchus: a systematic review. Clin Oncol (R Coll Radiol). 2002. 14:338–351.2. Doty DB, Doty JR, Jones KW. Bypass of superior vena cava. Fifteen years' experience with spiral vein graft for obstruction of superior vena cava caused by benign disease. J Thorac Cardiovasc Surg. 1990. 99:889–895. discussion 895-896.3. Armstrong BA, Perez CA, Simpson JR, Hederman MA. Role of irradiation in the management of superior vena cava syndrome. Int J Radiat Oncol Biol Phys. 1987. 13:531–539.4. Yellin A, Mandel M, Rechavi G, Neuman Y, Ramot B, Lieberman Y. Superior vena cava syndrome associated with lymphoma. Am J Dis Child. 1992. 146:1060–1063.5. Dyet JF, Nicholson AA, Cook AM. The use of the Wallstent endovascular prosthesis in the treatment of malignant obstruction of the superior vena cava. Clin Radiol. 1993. 48:381–385.6. Nicholson AA, Ettles DF, Arnold A, Greenstone M, Dyet JF. Treatment of malignant superior vena cava obstruction: metal stents or radiation therapy. J Vasc Interv Radiol. 1997. 8:781–788.7. Nagata T, Makutani S, Uchida H, Kichikawa K, Maeda M, Yoshioka T, et al. Follow-up results of 71 patients undergoing metallic stent placement for the treatment of a malignant obstruction of the superior vena cava. Cardiovasc Intervent Radiol. 2007. 30:959–967.8. Lanciego C, Pangua C, Chacon JI, Velasco J, Boy RC, Viana A, et al. Endovascular stenting as the first step in the overall management of malignant superior vena cava syndrome. AJR Am J Roentgenol. 2009. 193:549–558.9. Cheng S. Superior vena cava syndrome: a contemporary review of a historic disease. Cardiol Rev. 2009. 17:16–23.10. Nguyen NP, Borok TL, Welsh J, Vinh-Hung V. Safety and effectiveness of vascular endoprosthesis for malignant superior vena cava syndrome. Thorax. 2009. 64:174–178.11. Chin DH, Petersen BD, Timmermans H, Rosch J. Stent-graft in the management of superior vena cava syndrome. Cardiovasc Intervent Radiol. 1996. 19:302–304.12. Gill K, Ettles DF, Nicholson AA. Recurrent superior vena caval obstruction due to invasion by malignant thymoma: treatment using a stent-graft. Br J Radiol. 2000. 73:1015–1017.13. Azizzadeh A, Pham MT, Estrera AL, Coogan SM, Safi HJ. Endovascular repair of an iatrogenic superior vena caval injury: a case report. J Vasc Surg. 2007. 46:569–571.14. Mansour M, Altenburg A, Haage P. Successful emergency stent implantation for superior vena cava perforation during malignant stenosis venoplasty. Cardiovasc Intervent Radiol. 2009. 32:1312–1316.15. Martin M, Baumgartner I, Kolb M, Triller J, Dinkel HP. Fatal pericardial tamponade after Wallstent implantation for malignant superior vena cava syndrome. J Endovasc Ther. 2002. 9:680–684.16. Dartevelle PG, Chapelier AR, Pastorino U, Corbi P, Lenot B, Cerrina J, et al. Long-term follow-up after prosthetic replacement of the superior vena cava combined with resection of mediastinal-pulmonary malignant tumors. J Thorac Cardiovasc Surg. 1991. 102:259–265.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Superior Vena Cava Syndrome
- Bypass of Superior Vena Cava with Spiral Vein Graft
- Treatment of Superior Vena Cava Syndrome
- Dialysis Catheter-Related Superior Vena Cava Syndrome with Patent Vena Cava: Long Term Efficacy of Unilateral Viatorr Stent-Graft Avoiding Catheter Manipulation
- A Case of Behcet's Disease with Superior Vena Cava Syndrome
